Child malnutrition (including undernutrition and overweight)
National development is largely dependent on healthy and well-nourished people, but many children are not able at all times to access sufficient, safe, nutritious food and a balanced diet that meets their needs for optimal growth and development, an active and healthy life (UNICEF, 2013). Maternal and child malnutrition in low and middle income countries encompasses both under nutrition and a growing problem with overweight and obesity. Many countries are facing a double burden of malnutrition – characterized by the coexistence of undernutrition along with overweight, obesity or diet-related NDC – which poses a real and growing health challenge. The identification, promotion and implementation of actions that simultaneously and synergistically address undernutrition as well as overweight, obesity and diet-related NCDs are important opportunities and immediate priorities to foster the United Nations Decade of Action on Nutrition: food systems for healthy, sustainable diets; aligned health systems providing universal coverage of essential nutrition actions; safe and supportive environments for nutrition at all ages; social protection and nutrition-related education; trade and investment for improved nutrition; and strengthen and promote nutrition governance and accountability (WHO, 2017c).
Undernutrition is an important determinant of poor child health and is estimated to contribute to 45% of all child deaths worldwide (Black et al., 2013), although it is rarely listed as a direct cause. In order to reduce under age 5 mortality, countries need to not only implement effective preventive and curative interventions for newborns, children and their mothers during and after pregnancy (see indicator “Infant and child health” in Chapter 5) but also to promote optimal feeding practice (see indicator “Infant and young child feeding” in Chapter 4).
Child malnutrition also predicts poorer cognitive and educational outcomes in later childhood and adolescence and has important education and economic consequences at the individual, household and community levels. Obesity in adulthood is a major risk factor for the world’s leading causes of poor health and early death including cardiovascular disease, several common cancers, diabetes and osteoarthritis. Preventing obesity has direct benefits for children’s health and wellbeing, in childhood and continuing into adulthood (WHO, 2018b).
The UN SDG target 2.2 sets that “by 2030, end all forms of malnutrition, including achieving, by 2025, the internationally agreed targets on stunting and wasting in children under five years of age”, and also includes an indicator on childhood overweight. In 2012, the World Health Assembly endorsed a Comprehensive implementation plan on maternal, infant and young child nutrition, which specified a set of six Global Nutrition Targets by 2025 (WHO, 2014c): to achieve a 40% reduction in the number of children under age five who are stunted; to achieve a 50% reduction of anaemia in women of reproductive age; achieve a 30% reduction in low birth weight; ensure that there is no increase in childhood overweight; increase the rate of exclusive breastfeeding in the first six months up to at least 50%; and to reduce and maintain childhood wasting to less than 5%.
The recently released report of the commission on ending childhood obesity (WHO, 2016b) states that “Childhood obesity is reaching alarming proportions in many countries and poses an urgent and serious challenge”. And suggests that “obesity prevention and treatment requires a whole-of-government approach in which policies across all sectors systematically take health into account, avoid harmful health impacts, and thus improve population health and health equity”.
High levels of stunting in a country are associated with poor socioeconomic conditions and increased risk of frequent and early exposure to adverse conditions such as illness and/or inappropriate feeding practices (WHO, 2014d). Wasting may also be the result of a chronic unfavourable condition, like unsafe water and poor or lacking sanitary facilities. Recurrent events of wasting can increase the risk of stunting, and stunting increases the risk of overweight and obesity later in life.
Many countries in Asia-Pacific have a high prevalence of stunting and wasting among children under age 5. Stunting prevalence is high at around 43% or more in Papua New Guinea, Lao PDR and Pakistan, whereas it is below 5% in the Republic of Korea and Australia (Figure 4.9). As for wasting, if there is no severe food shortage, the prevalence is usually below 10% even in poor countries, but it is much higher than this threshold in some countries such as India and Sri Lanka (Figure 4.9). On average, one in three children under age 5 in lower-middle and low income Asia-Pacific countries have stunted growth, whereas one in ten children under age 5 present low weight-for-height. The stunting and wasting prevalence is much lower in upper-middle and high income Asia-Pacific countries at 11.7% and 7.1% for stunting and 6.3% and 2% for wasting respectively.
Countries with higher stunting prevalence have a higher under age 5 mortality rate (Figure 4.10), reflecting also the fact that about 43% of under age 5 deaths are attributable to undernutrition (Black et al., 2013).
Childhood overweight and obesity is one of the most serious challenges of the 21st century. Its prevalence has increased at an alarming rate and the number of overweight or obese children under age 5 is estimated to be over 41 million worldwide in 2016. Almost half of these children live in Asia (WHO, 2018b). The prevalence of childhood overweight varies across Asia-Pacific, with a prevalence of 4.7% and 6.5% across lower-middle and low income and upper-middle income countries respectively (Figure 4.11). More than one child out of ten is overweight in Mongolia, Indonesia and Papua New Guinee, whereas less than 2% of children under age 5 are overweight in Japan, Bangladesh, Myanmar and Nepal.
The WHO definition of children overweight is weight-for-height greater than 2 standard deviations above WHO Child Growth Standards median. The WHO definition of children obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median.
Stunted growth (low height-for-age) reflects failure to reach linear growth potential as a result of long-term suboptimal health and/or nutritional conditions.
Wasting (low weight-for-height) usually indicates recent and severe weight loss, because a person has not had enough food to eat and/or they have had an infectious disease, such as diarrhoea, which has caused them to lose weight.
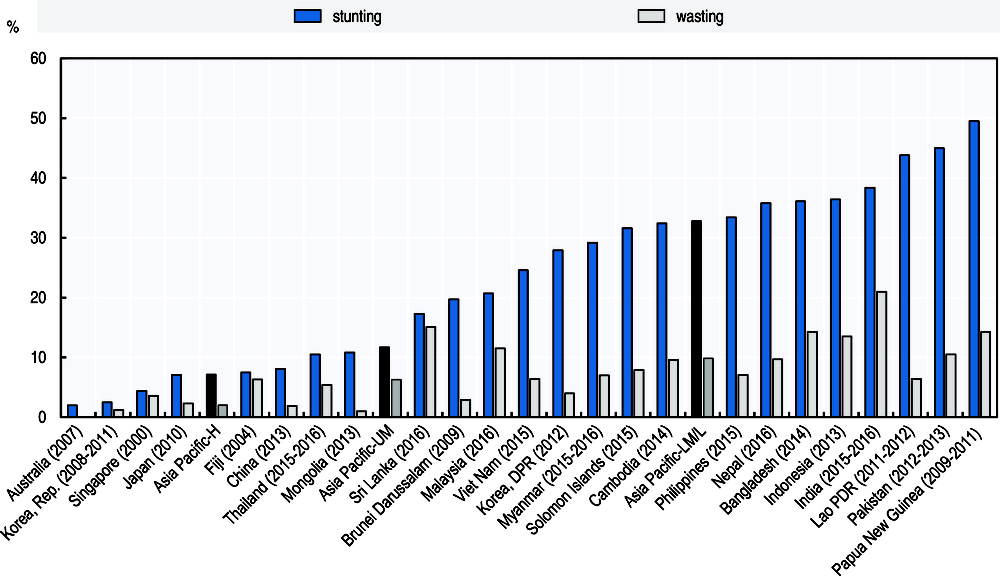
Source: WHO GHO 2018.
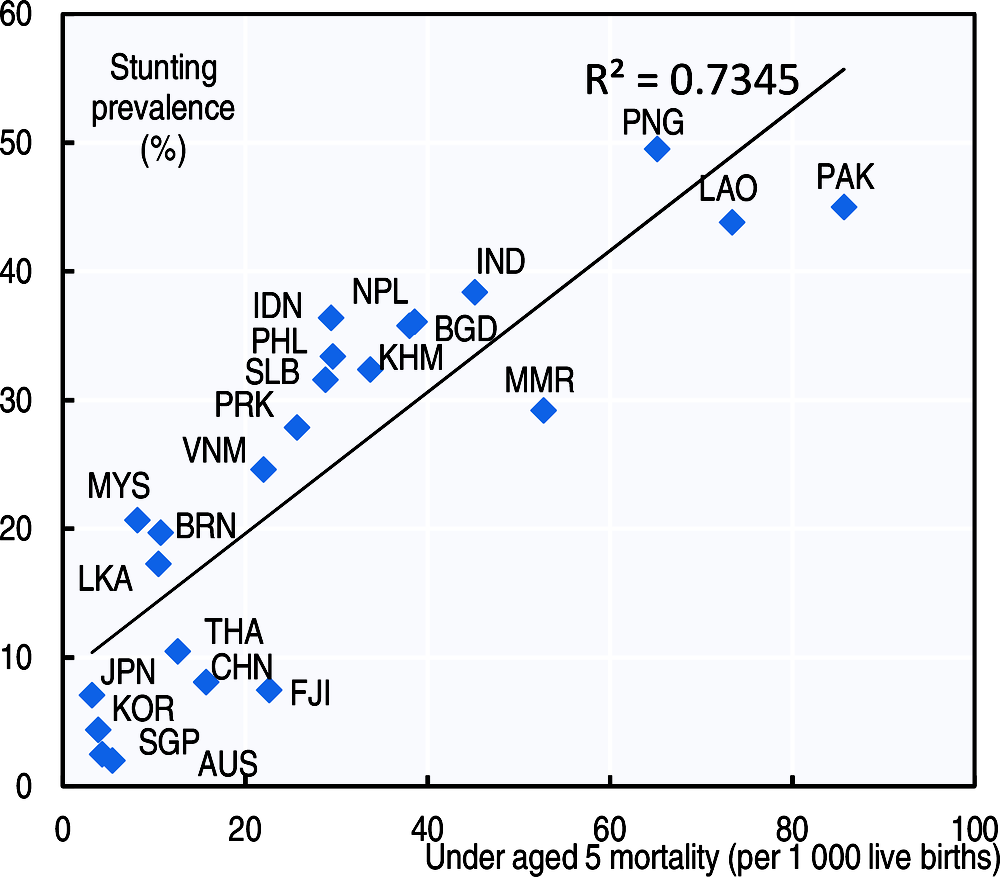
Source: WHO GHO 2018; UN IGME Childinfo. National survey on children for India for 2013-14.
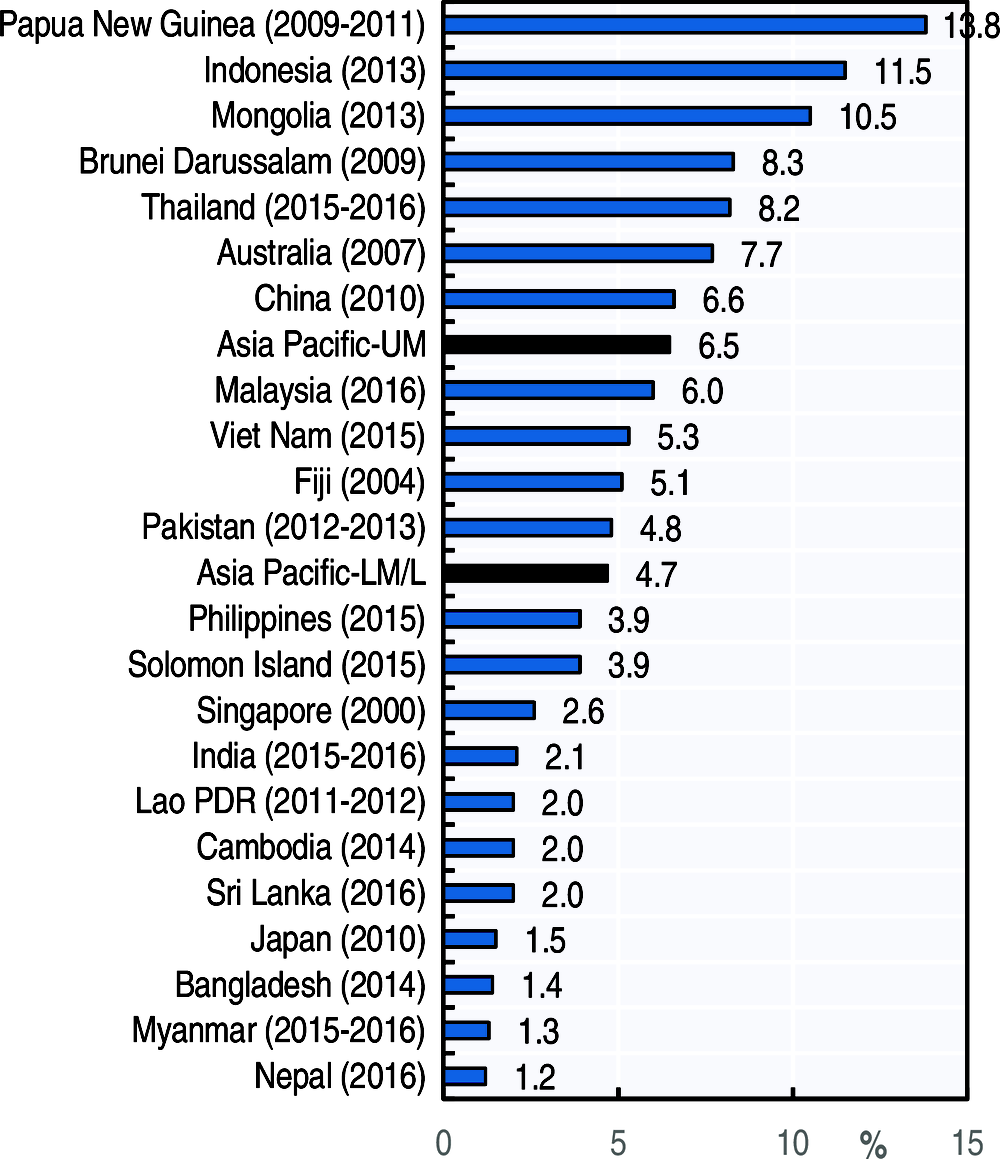
Source: WHO GHO 2018.