
Breast cancer care
Breast cancer is the cancer with the highest incidence among women in all OECD countries, and the second most common cause of cancer death among women (see indicator “Cancer incidence and mortality” in Chapter 3). Although the quality and outcomes of breast cancer care have generally been improving in recent years, as seen in improved survival estimates, the COVID-19 pandemic may have a negative impact on breast cancer outcomes in OECD countries.
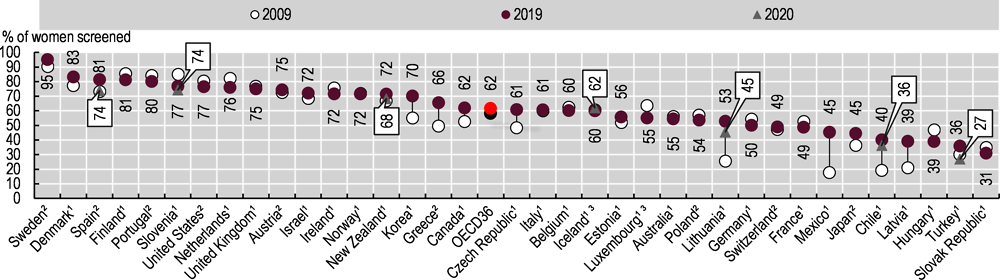
At the onset of the pandemic, many health systems prioritised urgent care needs, and cancer screening programmes were paused (OECD, 2021[6]). Many women also delayed seeking health care to reduce the risk of COVID-19 transmission, which led to a decline in breast cancer screening uptake in many OECD countries (see Chapter 2 “The Health Impact of COVID-19”; Figure 6.32). These changes will slow progress towards earlier diagnosis made in OECD countries that have adopted breast cancer screening programmes (OECD, 2013[43]), which led to an increase in the proportion of women of screening age receiving mammography from 57.3% in 2009 to 61.7% in 2019.
Changes in the stage of the disease at diagnosis can signal changes in timely access to high-quality breast cancer care. During 2010-14, 51.5% of women with breast cancer were diagnosed at an early stage and 8.6% at an advanced stage across OECD countries (Figure 6.33). During the COVID-19 pandemic, the stage distribution changed in several OECD countries. The Netherlands, where breast cancer screening was halted, for example, had a higher share of breast cancer patients diagnosed at the advanced stage during the first wave of the crisis in 2020 compared to the same period in the previous two years (NABON COVID-19 Consortium and the COVID and Cancer-NL Consortium, 2021[44]).
Delayed screening, diagnosis and treatment may lead to poorer outcomes for breast cancer patients in the near future. To minimise these consequences, a few OECD countries, such as Denmark, have made additional efforts to increase screening uptake and to reduce the backlog of cancer diagnosis.
The collection of patient-reported outcome measures (PROMs) in breast cancer care is growing; these can inform treatment choices and policy action to improve the quality of care services for breast cancer patients. Many OECD countries are scaling up their breast cancer PROMs initiatives to regional (e.g. Italy) and national (e.g. the Netherlands, Sweden) levels in order to make their health systems more people-centred.
The COVID-19 crisis has magnified the benefits to health systems of having systematic collection of PROMs in place. The pandemic has challenged health systems to deliver more timely and appropriate breast cancer care in a few OECD countries. Evidence shows that, from the onset of the pandemic, breast cancer patients and survivors were less likely to contact physicians, and experienced a deterioration in their emotional functioning and mental health (Bargon, 2021[45]). With the aim of minimising surgical complexity, length of stay, complication risks and the risk of COVID-19 infection, some countries and certain hospitals – including Sweden, the United Kingdom and the U.S. Brigham and Women’s Hospital – reduced or suspended all immediate breast reconstruction surgery and delayed reconstruction to be offered once services returned to normal (Dave, 2021[46]; Regionala Cancercentrum I Samverkan, 2021[47]). Such disruptions in care have significantly affected the ability for participating hospitals to deliver PROMs data to the OECD.
Figure 6.34 presents crude (unadjusted) breast satisfaction outcome scores at 6-12 months following breast cancer procedures (breast-conserving therapy and reconstruction following mastectomy) for ten clinical sites in nine countries. Results suggest higher breast satisfaction outcomes after breast-conserving therapy in some, but not all, sites. Consolidated mean crude scores from all 10 sites except Switzerland show higher breast satisfaction scores following breast-conserving therapy compared to reconstruction surgery.
Cancer patient data were provided by national or regional cancer registries. Screening rates are based on survey or programme data. Survey-based results may be affected by recall bias. Quality control, analysis of stage distribution and estimation of age-standardised five-year net survival were performed centrally as part of CONCORD, the global programme for the surveillance of cancer survival, led by the London School of Hygiene and Tropical Medicine (Allemani et al., 2018[48]). The stage at diagnosis for breast cancer is categorised according to the Tumour, Nodes, Metastasis staging system.
PROMs data are only presented for selected hospitals and are not representative for each country. Outcomes were measured using the relevant postoperative breast satisfaction scales from the BREAST-Q tool, an internationally validated instrument used to measure breast surgery outcomes reported by patients (Pusic et al., 2009[49]). A higher score denotes better outcomes.
Caution is advised when comparing the results of participating sites for several reasons. The size of participating programmes in terms of patient numbers varied considerably from regional efforts to single hospitals. These differences are reflected in the confidence intervals included in Figure 6.34. Note that measurement extended beyond 12 months after surgery for some sites. Data from Flinders Medical Centre (Australia), University of Western Australia Medical School (Australia), Portugal (Site A), 12 Octubre Hospital (Spain) and Brigham and Women’s Hospital (United States) are not included in the figure due to small sample sizes. Data from these sites, and additional data on the sites and samples can be found in a forthcoming technical report.

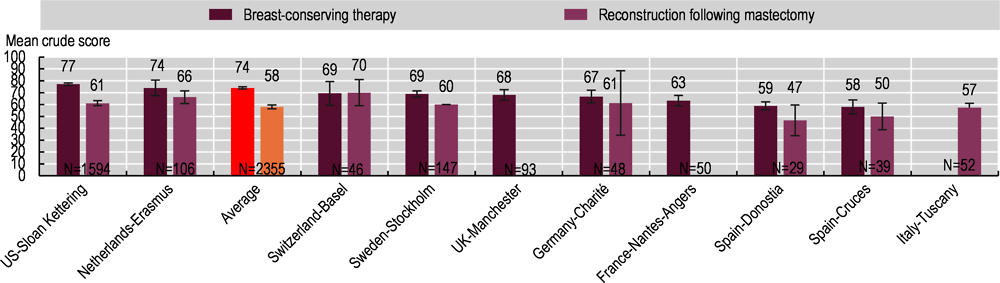
Note: H lines show 95% confidence intervals. Weighted average based on site sample size was used to calculate crude average breast satisfaction. Data labels at the base of the histogram refer to the sample size at each site.
Source: PaRIS Breast Cancer PROMs pilot data collection 2021.