
copy the linklink copied!2. Tackling harmful alcohol use
Harmful alcohol use is a considerable public health issue in Korea. Alcohol plays an important part in daily life and binge drinking is common. While some policies have been introduced to reduce harmful alcohol consumption – including taxation, labelling, drink-driving regulation and education in universities – there remains scope to improve. Implementing a comprehensive policy package, which includes stricter marketing regulation, regulation on the sale and consumption of alcohol, education and public awareness programmes among all levels of society as well as improved pricing policies, can help tackle harmful alcohol consumption in Korea.
copy the linklink copied!Introduction
The amount of alcohol consumed in Korea is similar to the OECD average – but this overall trend obscures the issues that exist around harmful alcohol use. Working men and young women are frequent drinkers; binge-drinking is common and socially accepted – if not encouraged; alcohol dependency rates are high; and there are more alcohol-related road traffic crashes per capita than in any other OECD country.
To address these issues, Korea has implemented a number of policies, including awareness and education campaigns, taxation, some regulation of advertising, warning labels on alcohol containers, and a national maximum legal blood alcohol concentration for drivers linked to monetary fines or imprisonment.
Despite these efforts, the social acceptability of excessive alcohol use remains high in Korea. This is turn hampers the implementation of more progressive alcohol legislation, which often lacks public and political support. For this reason, it is crucial to change the current social acceptability of harmful alcohol consumption, and pave the way for more comprehensive policies.
This chapter will first describe the levels and patterns of alcohol use in Korea, and the impact it has on society and the economy. Secondly, it will describe the current alcohol prevention strategy that is in place in Korea. Thirdly, it will outline additional policies that Korea should consider implementing to tackling the problem of harmful alcohol use.
copy the linklink copied!2.1. Harmful alcohol use is a public health issue in Korea
2.1.1. Although the overall alcohol consumption rate in Korea is around OECD average, working men and young women are frequent drinkers
Compared to recorded alcohol consumption in other OECD countries, Korea consumes a similar amount: 8.7 litres per capita compared to 8.9 on average in the OECD (see Figure 2.1). This level of consumption has remained largely stable over the past two decades. Unrecorded alcohol consumption in Korea is estimated at 1.2 litres per capita (World Health Organization, 2018[1]). This is below the OECD average of 1.4 litres. (Please refer to Box 2.1 for details on measuring alcohol consumption and the differences between OECD and WHO data).
There are different ways of measuring alcohol consumption in a country. The WHO Global Information System on Alcohol and Health (GISAH) database contains both recorded and total consumption. Recorded alcohol consumption only takes into account the consumption that is recorded from production, import, export, and sales data, often via taxation. Total alcohol consumption also looks at unrecorded (and untaxed) alcohol and subtracts the amount of alcohol consumed by tourists (World Health Organization, n.d.[2]). Unrecorded alcohol is not included in official statistics because it is produced, distributed and sold outside the formal channels under government control.
The OECD also reports data on recorded alcohol consumption in its Health Statistics. For some countries GISAH data is used, while for others data is supplied to the OECD by the country government. When considering just recorded alcohol consumption, estimated from OECD Health Statistics data and WHO GISHA data are very close. Exceptions are Estonia, Lithuania, Czech Republic, Russia, and Mexico. Generally, these differences are due to adjustments or differences in methodology. In Estonia, the OECD uses the government figure, which includes a correction for tourist consumption and illegal alcohol. In the Czech Republic, the government methodology also differs from the WHO, notably on the degree of alcohol in beer.
The Health Statistics data presented in this publication is different from the data in the OECD’s forthcoming (2020) report on harmful alcohol consumption because that report primarily uses total alcohol consumption instead of recorded alcohol consumption, as in this publication.
Sources: World Health Organization (n.d.[2]), Alcohol, total per capita (15+ years) consumption (in litres of pure alcohol), https://www.who.int/data/gho/indicator-metadata-registry/imr-details/465; World Health Organization (2018[3]), WHO Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en.
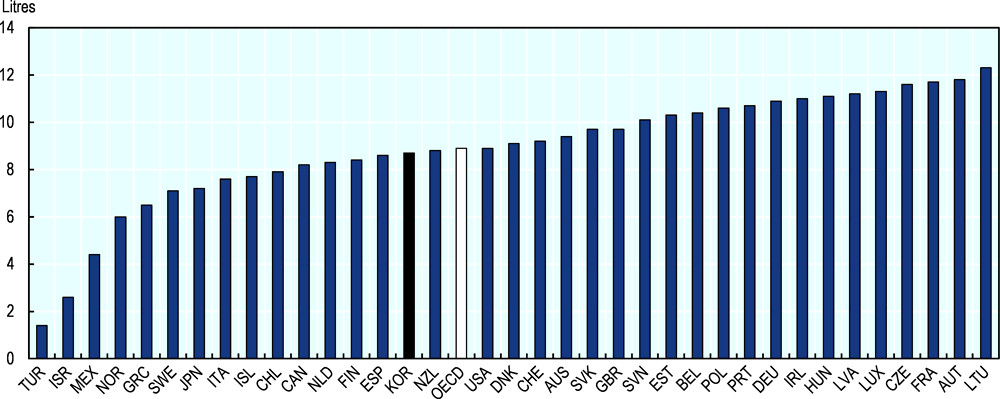
Note: Please refer to Box 2.1 for details on alcohol consumption data and the differences between OECD and WHO data.
Source: OECD (2019[4]), OECD Health Statistics 2019, http://stats.oecd.org/.
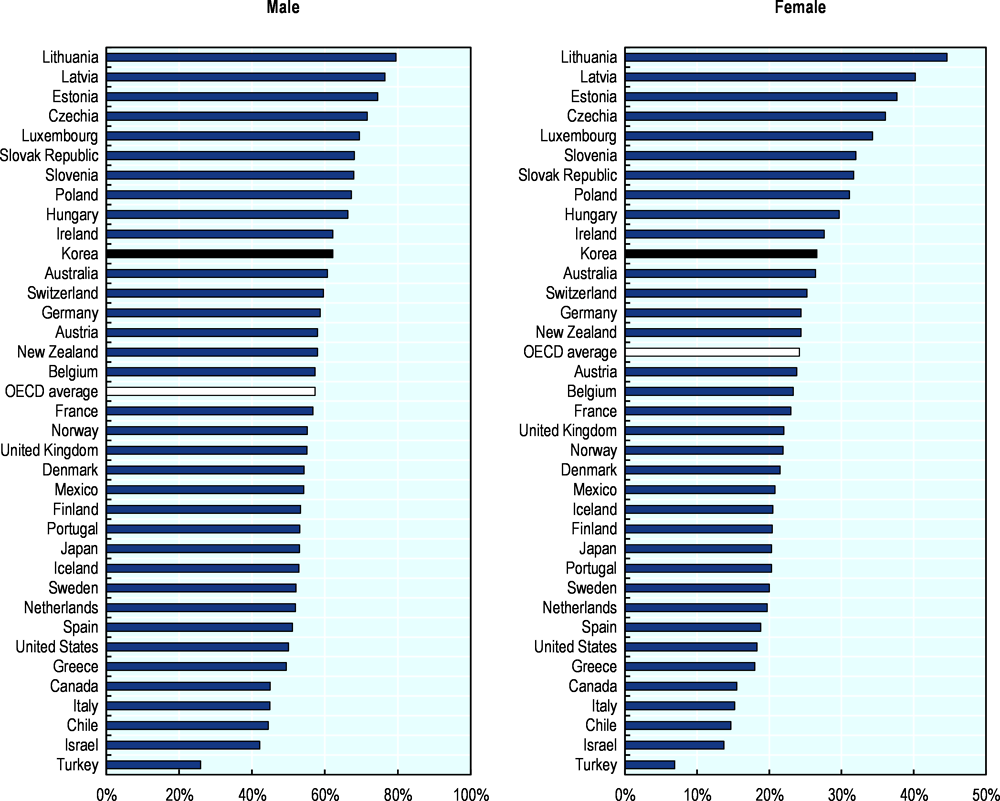
Alcohol consumption is not evenly distributed across the Korean population, as men consume more alcohol than women. Among those who drink, total alcohol consumption is 21.7 litres per year for men compared to 7.6 litres for women (World Health Organization, 2018[1]). However, alcohol consumption among women has increased considerable in recent years: while in 1992 33% of women over 20 drank alcohol (compared to 84.7% of men), this had increased to 59.5% in 2001 (Kim and Kim, 2008[5]). More recent data indicates that in 2014, 60% of women drank, compared to 75% of men (KNHANES, 2019[6]). Like in other cultures, traditionally women were expected to refrain from drinking. However, with changing social norms and the increased participation of women in the workforce this has started to change (Kim and Kim, 2008[5]).
For both men and women, regular alcohol consumption is most common in middle age (see Figure 2.2). However, for men the frequency of drinking remains relatively high in older age, with 29% of men over the age of 75 consuming alcohol at least twice a week.
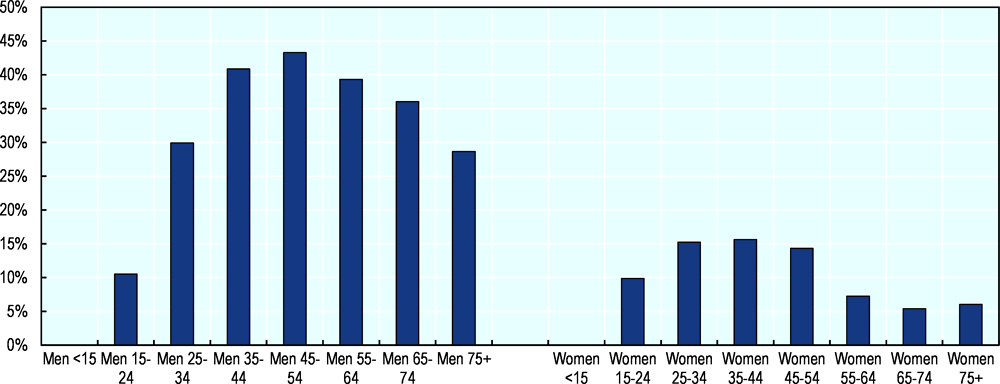
Source: KNHANES (2019[6]), Korea National Health and Nutrition Examination Survey, https://knhanes.cdc.go.kr/knhanes/sub01/sub01_02.do.
The legal drinking age in Korea is 19 years old. Nevertheless, nearly half of all 16 year olds have drunk alcohol at least once (see Figure 2.3). Moreover, by the age of 16 over 20% of children drink alcohol at least once a month, rising to nearly 30% at age 18 (KCDC, 2017[7]).
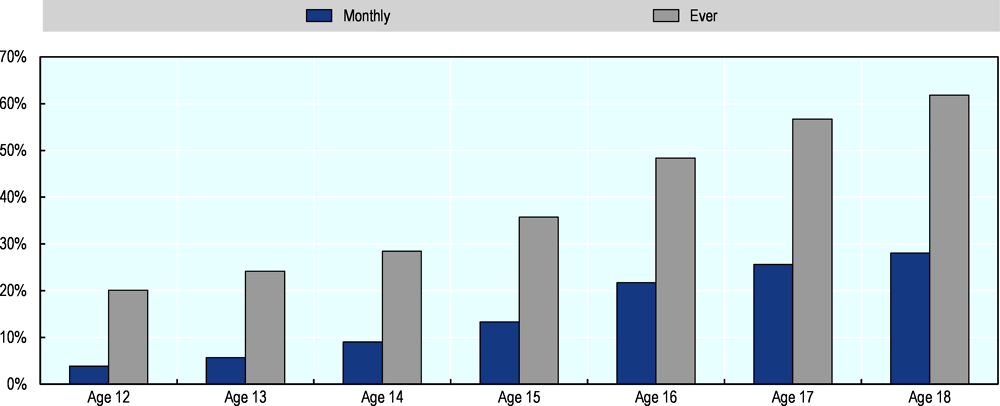
Source: KCDC (2017[7]), Youth Health Behavior Survey, http://www.cdc.go.kr/CDC/contents/CdcKrContentView.jsp?cid=77749&menuIds=HOME001-MNU1130-MNU2393-MNU2749.
The frequency of drinking in men is lower in population groups with higher education (see Figure 2.4). Nearly 40% of men with a low educational level drink at least twice a week, compared to less than one third of men with a high educational level. On the other hand, women with a low education are less likely to drink frequently compared to those with a medium or high educational level.
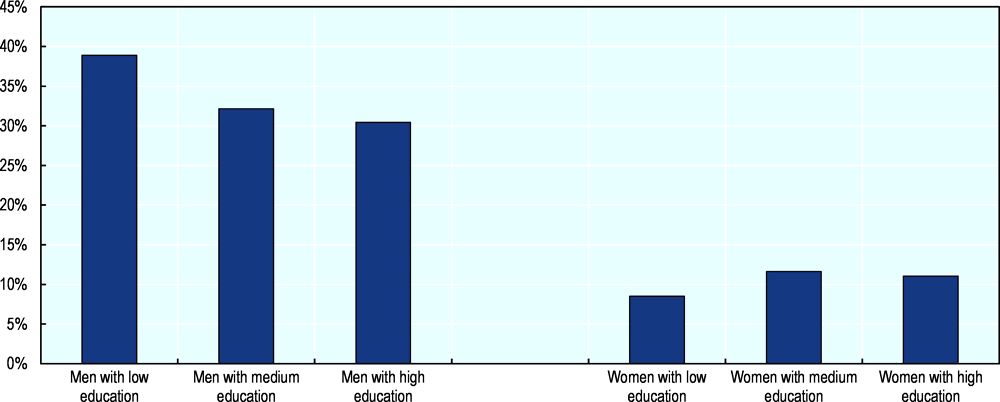
Source: KNHANES (2019[6]), Korea National Health and Nutrition Examination Survey, https://knhanes.cdc.go.kr/knhanes/sub01/sub01_02.do.
Occupational status is another important determinant of drinking status in Korea (see Figure 2.5). Men who work are much more likely to drink at least twice a week compared to men who do not work. For women the same effect can be observed though at a lower overall level.

Source: KNHANES (2019[6]), Korea National Health and Nutrition Examination Survey, https://knhanes.cdc.go.kr/knhanes/sub01/sub01_02.do.
Beer and soju are the most popular drinks in Korea, accounting for approximately 60% and 25% of overall litres consumed respectively (USDA Foreign Agricultural Service, 2018[8]). Soju is a traditional distilled spirit with typically about 20-24% alcohol by volume (ABV). Its popularity in Korea means that it is one of the most consumed liquors worldwide (Drinks International, 2016[9]).
In recent years there has been an increase in the production, marketing and consumption of fruit-flavoured drinks and drinks with a lower alcohol percentage. The preference for liquors low in alcohol content has increased from 53.7% in 2013 to 57.0% in 2016 (Ministry of Drug and Food Safety, 2016[10]). This trend is driven in particular by young women.
Craft and international beers are also gaining popularity, driven by an increased consumer demand for quality and diversity. The total volume of beer imports increased by 50% between 2016 and 2017. Nevertheless, the market for beer remains highly consolidated: two national brewers account for 86% of beer sales in 2017 (USDA Foreign Agricultural Service, 2018[8]).
2.1.2. Heavy episodic and high-risk drinking is common in Korea
While the overall rates of alcohol use in Korea are around the OECD average, the rate of heavy episodic drinking, or binge drinking, is high (see Figure 2.6). The average number of drinks consumed in one sitting has almost tripled from 2.2 cups in 2013 to 6.0 cups in 2016 (Ministry of Drug and Food Safety, 2016[10]). This is important since heavy episodic drinking is harmful to a person’s health even if the overall level of alcohol consumption is low. Moreover, in the presence of heavy episodic drinking, the cardioprotective properties of low-risk alcohol consumption disappear completely (World Health Organization, 2014[11]).
Source: World Health Organization (2018[3]), Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en.
The prevalence of heavy episodic drinking, measured as the percentage of the men who consume 7 cups of alcohol or more in one drinking event at least once a month, or 5 cups or more for women, is a particularly high among younger people and adult men (see Figure 2.7). More than half of all men below the age of 59 binge drink at least once a month. While the overall prevalence of heavy episodic drinking in women is lower, nearly half of women aged 19-29 engages in monthly binge drinking.
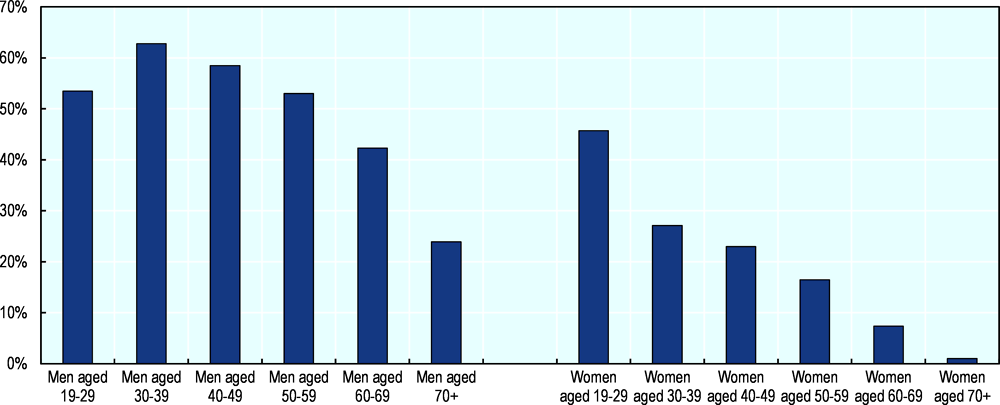
Source: Korean National Health Statistics (data supplied to the OECD by the Ministry of Health and Welfare).
When it comes to high-risk drinking, defined as engaging in heavy episodic drinking at least twice a week, men between the ages of 30 and 59 have the highest rates of around 25% (see Figure 2.8). The prevalence of high-risk drinking is lower in women, with the highest rate in women between 19 and 29 years old.
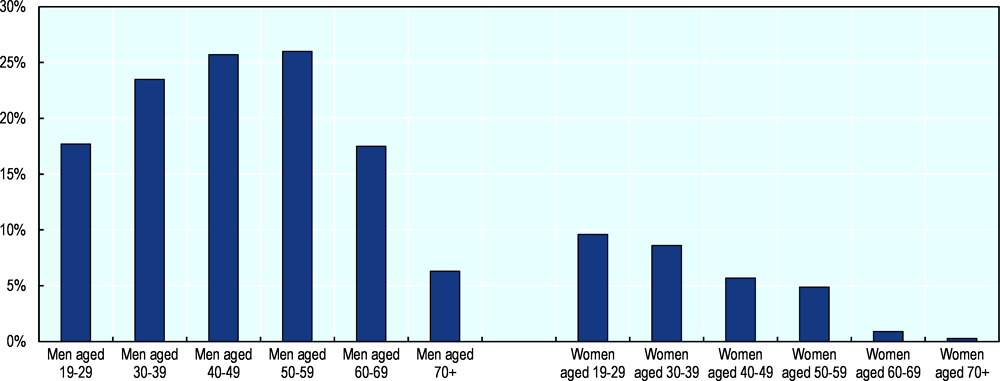
Source: Korean National Health Statistics (data supplied to the OECD by the Ministry of Health and Welfare).
An important contributor to the high rate of harmful alcohol consumption in Korea is the drinking culture, which is conducive to heavy episodic drinking (see Box 2.2).
In Korea, the consumption of alcohol is an important part of social interactions, in particular in the workplace (Jun and Chung, 2008[12]). Employees go out regularly for team dinners, which often involve large quantities of alcohol and drinking games. Alcohol is thought to help overcome the barriers of work hierarchy and contribute to the creation of closer interpersonal relationships. Others see it as a way to cope with the high workload and long working hours that are typical of Korean office jobs.
The same social expectations around alcohol also affect other population groups, for example college students. Between 40% to 80% of college students is estimated to be a problem drinker (Kim and Park, 2015[13]), and studies have shown that social bonding and peer pressure are major drivers of alcohol misuse in this group – more so than in other cultures (Kim, Ahn and Lim, 2015[14]).
Traditional customs further contribute to the high intake of alcohol during social gatherings. It is considered impolite to refuse a drink, especially if offered by a superior, and to leave someone else’s glass empty. Soju is usually sold in 375 millilitre bottles, which are shared among groups in small shot glasses that are regularly topped up.
The social acceptance of alcohol is also partially reflected in the regulation of consumption and in the social acceptability of drunkenness. Regulations of sales and consumption of alcohol product is much weaker in Korea than in many other OECD countries. Korean society and law enforcement are generally tolerant to public drunkenness. In fact, drunkenness is considered a mitigating circumstance for acts of violence, and can be cause for leniency in sentencing. There have however been calls to change this approach (Korea Times, 2017[15]).
Sources: Korea Times (2017[15]), Anger growing against alcohol-influenced crimes, http://www.koreatimes.co.kr/www/nation/2017/12/356_240362.html; Jun and Chung (2008[12]) “Effects of Workplace Alcohol-related Environment on Drinking Behaviors among Female Employees”, Korean Journal of Health Education and Promotion, Vol. 25/3, pp. 21-43, http://linkinghub.elsevier.com/retrieve/pii/S0306460304000747; Kim, J. and S. Park (2015[13]), “Association between protective behavioral strategies and problem drinking among college students in the Republic of Korea”, Addictive Behaviors, Vol. 51, pp. 171-176, https://doi.org/10.1016/J.ADDBEH.2015.07.017; Kim, S., S. Ahn and T. Lim (2015[14]), “Predicting Alcohol Misuse Among College Students in the US and South Korea”, Journal of Ethnicity in Substance Abuse, Vol. 14/3, pp. 308-322, https://doi.org/10.1080/15332640.2014.996313.
2.1.3. Alcohol use has a considerable impact on Korean health and society
Harmful alcohol use negatively affects population health in Korea. For men, 6.7% of all deaths can be attributed to alcohol use in 2016 (GBD 2016 Alcohol Collaborators, 2018[16]). For women this is 2.2% of deaths. As such, alcohol is the third major behavioural risk factor, after tobacco use and dietary risk (Institute for Health Metrics and Evaluation, 2017[17]). It is responsible for 33% of all deaths from oesophageal cancer, 15% of deaths from liver cancer, 17% of deaths from breast cancer, 41% of deaths from chronic liver diseases (including cirrhosis), and 20% of deaths from self-harm.
The prevalence of alcohol dependency in Korea is relatively high compared to other OECD countries (see Figure 2.9), and this figure has grown in recent years. The number of persons seeking medical care for alcohol use disorders has also increased, growing over 50% between 2002 and 2013, from 73 000 to 114 000 (though it is unclear whether this is only due to an increase in prevalence, or whether this is also driven by an increase in access to treatment). The associated medical cost more than tripled from KRW 120 billion to KRW 375 billion over the same period (Korea Institute of Health and Social Affairs, 2017[18]).
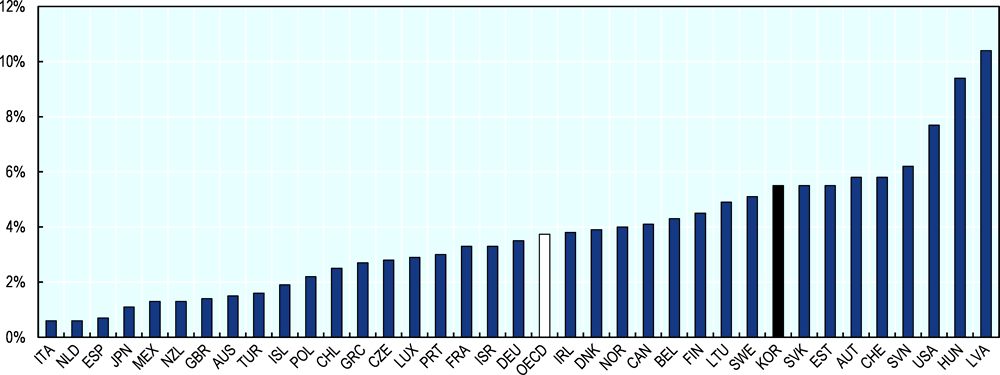
Source: World Health Organization (2018[3]), Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en.
In addition to alcohol use disorders, alcohol consumption also causes other health issues, including cancers, cardiovascular diseases and liver disease, and contributes to the rate of injuries and suicides. The Korea Institute for Health and Social Affairs estimates the total cost of illnesses attributable to at-risk (drinking three to four times a week) and high-risk (drinking almost every day) alcohol use at KRW 4.6 trillion, of which KRW 1.0 trillion in medical expenses and KRW 2.9 trillion in lost income due to premature death (Korea Institute of Health and Social Affairs, 2017[18]). The cost of alcohol-attributable injuries and suicides contributes another KRW 1.5 trillion in lost income.
Furthermore, alcohol use contributes to crime and road traffic accidents. Korea has one of the highest rates of road traffic crashes due to alcohol (see Figure 2.10). Overall, alcohol consumption is responsible for 10.8% of all road traffic crashes in Korea (World Health Organization, 2017[19]). When it comes to violent crime, more than 30% of incidents is committed under the influence of alcohol (KIHASA, 2016[20]).

Note: Based on countries with available data and showing 2016, or the most recent year for which data is available.
Source: World Health Organization (2018[3]), Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en.
copy the linklink copied!2.2. Korea has in place a multifaceted alcohol prevention strategy
2.2.1. Organisation of alcohol prevention
In the Ministry of Health, the majority of work on alcohol prevention falls under the Mental Health Policy division, and the Department of Health Promotion. They are in charge of national regulation on packaging and advertising. The Ministry also works with the Korea Health Promotion Institute to run promotional campaigns and develop local health promotion plans. In addition, the Ministry of Food and Drug Safety is in charge of regulating the production and content of alcohol products; and the Ministry of Strategy and Finance manages alcohol taxation, distribution and sales.
Locally, Public Health Centers deliver health promotion and preventive care to their communities. Addiction Management Centers provide treatment for alcoholism and other addictions in a community center, but also play an important role in educating the community through outreach programmes and local campaigns.
The alcohol prevention strategy is set by the Ministry of Health. The first strategy was launched in 2006. The Bluebird Plan 2010 set out the Korean strategy on alcohol prevention until 2010, focusing on improving awareness, reducing harmful alcohol consumption and improving treatment. However, it has been suggested that the impact of the Bluebird Plan was limited, as it did not receive adequate budgets and failed to set up longer term action plans (Kim et al., 2013[21]). Since then, the strategy on alcohol prevention has been included in the five-year National Health Promotion Plan.
Most of the regulation on alcohol use is anchored in the Health Promotion Act, as well as topic specific acts, such as the Liquor Tax Act and the Road Traffic Act.
2.2.2. Awareness and education
The Korea Health Promotion Institute (KHPI) plays a central role in public awareness and education, as it runs national awareness campaigns and supports health promotion activities by Public Health Centers. In November, it coordinates the alcohol awareness month, providing materials for local interventions, web-tools and a national campaign to “re-start”.
There is no national alcohol-specific educational campaign for schools. Students receive health education, and while education on alcohol use is part of this curriculum, the primary focus is on tobacco. The Ministry of Health is looking to strengthen its alcohol education in schools and secure dedicated funding. Public Health Centers or Addiction Centers do provide materials and education in schools but only on an ad-hoc basis. Similarly, the KHPI has materials and trains instructors, but these are only provided at the schools’ request. A 2017 survey of youth showed that 58% of students did not receive alcohol education in the preceding 12 months (KCDC, 2017[7]).
In universities, student supporters play a role in raising awareness around harmful alcohol use. Since 2005, the Ministry of Health and Welfare has run a national programme to train and support students to act as moderate drinking supporters. In 2018, teams of students from 44 universities came together for an opening ceremony, where they received training, materials and mentoring in order to deliver prevention and education activities on their campuses (Korea Health Promotion Institute, 2018[22]). At the end of the year, a competition awards nine teams with scholarships.
In addition, a Moderate Drinking Code for college students was developed by the Ministry of Health and Welfare in 2018, and disseminated to 300 universities across the country. The Moderate Drinking Code advises students not to consume “bomb” drinks that combine soju and beer, not to force others to drink and not to drink shots or shout “bottoms up”, amongst others. It also recommends abstinence for people who experience an alcohol flush reaction (turning red in the face) – as well as people under the age of 19, pregnant women or women trying to get pregnant, and people on medication.
Workplace-based interventions exist that target drinking among employees and after work. The Ministry of Health is implementing a programme to promote cultural activities (such as a movie night) as company outings rather than drinking. The KHPI has created materials for companies to educate their staff on harmful drinking, but this is provided on request rather than systematically.
Local initiatives also try to address the workplace drinking culture. Some organisations, including Seoul City Hall and one of the major chaebol (business conglomerate) in the country, have adopted the “119 plan”. This slogan advises employees to have only one type of drink, at only one venue, and to go home before 9pm. Variations on this campaign are the “829 plan” which recommends finishing a work drinking outing between 8 and 9 pm, and the “222 plan”, which advised not to mix two kinds of alcohol, not to offer more than two shots to others and not to go to a second venue.
Both the KHPI and local Alcohol Addiction Centers produce leaflets that specifically focus on how to deal with social pressures to consume alcohol. Young people are advised to clearly state that they do not drink, to change the topic of conservation or to keep away from situations in which alcohol is consumed. Adults are also advised to avoid drinking, not to consume shots and “bomb drinks” (mixing soju and beer), and not to force others to drink.
2.2.3. Pricing
Korea levies excise taxes on alcoholic beverages, as decreed by the Liquor Tax Act. Until recently, alcoholic beverages were taxed based on the price set by the manufacturer (ad valorem), with the exception of spirits, which are taxed based on their volume (see Table 2.1).
However, the government has recently revised the tax structure and introduced a tax based on volume rather than value (The Korea Herald, 2019[24]). At first, the change only applies to beer and rice wine. The aim of this change is to address inequalities in tax rates between domestic and international brands. While for domestic beer brands the 72% tax rate was based on manufacturing costs, profit as well as selling, general and administrative expenses, the tax for foreign beer brands was only applied to import price and tariffs (Korea Times, 2019[25]). Under the new system, both domestic and foreign beer brands are taxed 830.3 won per litre. As a result, the retail price of domestic beer is expected to decrease (The Korea Herald, 2019[24]).
In addition to liquor tax, the amount of liquor tax payable is itself taxed with an education tax, at 30% for liquors taxed more than 70% and 10% for all others (Statutes of the Republic of Korea, n.d.[26]). The aim of this education tax, which is also applied to revenue earned by financial or insurance business entities, consumption tax, traffic, energy, and environment tax, is to secure funding for education and to improve the quality of the schooling system.
Korea has implemented measures to promote traditional liquor industries and enhance the competitiveness of Korean traditional liquors abroad (Statutes of the Republic of Korea, n.d.[27]). In addition to assistance, education, training and certification schemes to maintain the traditions, tax rates are reduced by 50% for up to 200 kilolitre1 of “traditional liquor”, when manufactured by holders of a national intangible culture heritage or food grand master appellation (Statutes of the Republic of Korea, 2009[23]).
Despite the liquor and education tax, alcoholic beverages in Korea remain relatively cheap. While prices for carbonated drinks, fruit juice and coffee increased by 208%, 61% and 57% respectively between 2005 and 2018, the prices of alcohol drinks increased between 4% and 36%, depending on the type of alcohol product (see Figure 2.11) (Korea Health Promotion Institute, 2019[28]). This is below inflation, as measured by the consumer price index.
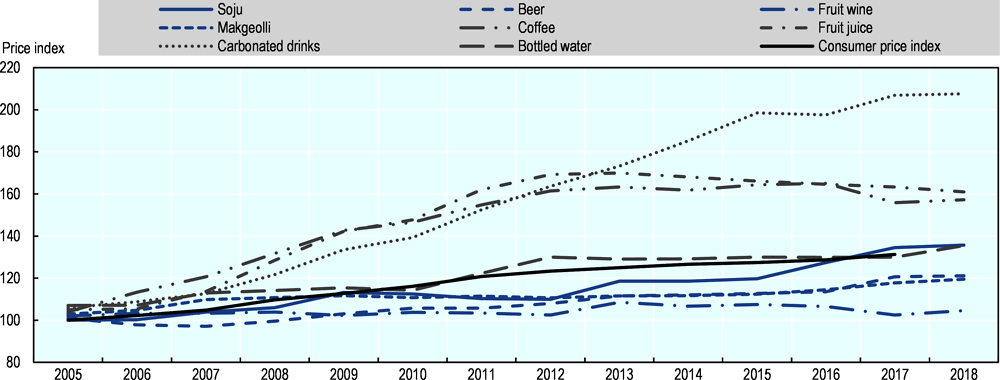
Note: Indexed at 2005 = 100; alcoholic drinks in black, non-alcoholic drinks in blue.
Source: Price data from Korea Health Promotion Institute (2019[28]), Price Index of Mainstream Liquor, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00688&tableGubun=DATA040401; consumer price index from OECD Inflation (CPI).
The popular soju is particularly inexpensive. A 360 millilitre bottle costs around KRW 1 340, or USD 1.15 (Korea Consumer Agency, 2019[29]). At 20% ABV, a bottle of soju provides 7.2 units2 of alcohol. Per comparison, this translates to an alcohol unit price of GBP 0.12 (USD 0.15), far below the GBP 0.50 (USD 0.64) minimum price that Scotland, Wales and England are considering (Financial Times, 2018[30]; Scottish Government, 2017[31]; Angus et al., 2017[32]). One of the reasons for this is its low production cost, around KRW 400 per bottle (Korea Herald, 2012[33]; Korea Expose, 2018[34]). These low prices mean that the ad valorem excise tax has less impact on the final sales price.
Overall, the low prices in Korea make alcohol easy accessible and affordable for a large part of population, contributing to an environment which is conducive to the consumption of alcohol.
2.2.4. Advertising and media
Advertising on traditional mass media primarily uses cable TV (see Figure 2.12). Between 2010 and 2018, the annual number of advertisements shown on cable TV increased by 17% per year, from 123 304 advertisements to 443 585 in 2018 (Korea Health Promotion Institute, 2019[35]).
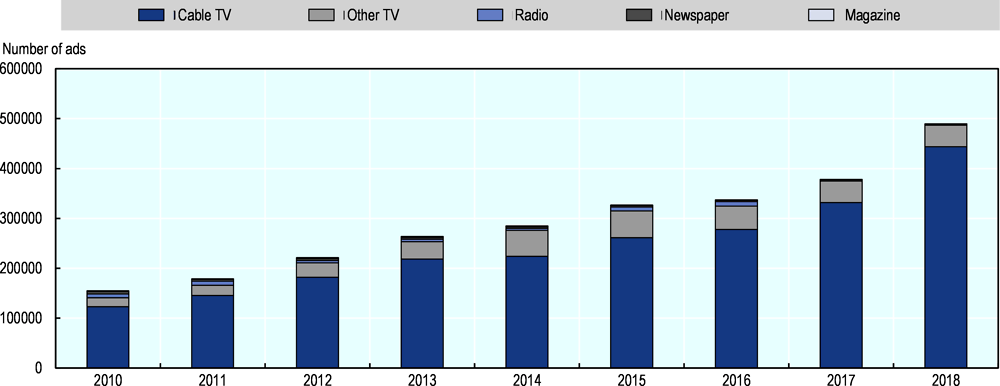
Source: Korea Health Promotion Institute (2019[35]), Annual Frequency of Alcohol Advertising, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00690&tableGubun=DATA070101.
Spending on alcohol advertisement in traditional mass media has grown by 13% per year over the same period (Korea Health Promotion Institute, 2019[36]). The majority of advertising spend is for beer, with soju in a distant second place (see Figure 2.13). Beer advertising grew by 18% per year, from KRW 59 billion in 2008 to KRW 312 billion in 2018.

Source: Korea Health Promotion Institute (2019[36]), Annual Expenditure on Alcohol Advertising, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00691&tableGubun=DATA070201.
In Korea, there exist some regulation on the content of alcohol marketing, and on the time and place of such marketing. Alcohol advertisements are not allowed to depict pregnant women, or adolescents, and alcohol containers must have a warning text. There have been attempts to extend the latter to ban the use of celebrities and models to promote drinks, but no law has been passed yet (European Centre for Monitoring Alcohol Marketing, 2019[37]).
Broadcast advertising of alcohol products with more than 17% alcohol is prohibited. Marketing and advertising of alcohol products with less than 17% ABV on television is restricted to after 10pm and before 7am. Similar restrictions apply to radio advertisements. However, this regulation only concerns targeted advertisements during commercial breaks. There is no regulation on the depiction of alcohol in television series and programming. Indeed, many Korean television shows contain frequent depictions of drinking, which are displayed as social, fun and desirable (The Korea Herald, 2017[38]). While programmes rated appropriate for audiences aged 19 and over can only be broadcast between 9am and 1pm on weekdays, and 10pm to 7am, programming rated 15+ can be aired anytime as long as a warning label is shown at the beginning. Voluntary guidelines are being developed to regulate television programming content.
There is no national regulation of other forms of alcohol advertising. Alcohol marketing can be seen on billboards, public transport and at retailers and catering. In addition, alcohol producers use social media to promote their products. The Ministry is looking to reform this, and has banned alcohol marketing through video clips shown on trains.
Together, the limited regulations on alcohol marketing and the positive depictions of drinking can normalise and encourage drinking (Institute of Alcohol Studies, 2019[39]), reinforcing the social acceptability towards harmful alcohol drinking that exists in Korea.
Monitoring is done by the KHPI. The KHPI checks the contents of advertisements on TV, radio, internet, newspapers, magazines, outdoor, subway and in theatres against the regulation set out in the Enforcement Decree of the National Health Promotion Act. It also flags the depiction of excessive drinking in TV programmes, and monitors the use of warning phrases (Korea Health Promotion Institute, 2017[40]). They identify about 10-15 violations per week, and after flagging the findings with the offending company they monitor any follow-up actions taken. If no actions are taken, the Ministry of Health can fine the offender for up to KRW 1 000 000 (Korea Health Promotion Institute, 2019[41]).
2.2.5. Labelling
In 2016, Korea revised the warning phrases that are required to be printed on the label of alcoholic products with more than 1% ABV. Producers can choose between three versions, all of which describe the risks of drinking during pregnancy as well as excessive drinking:
-
“Drinking during pregnancy increases the risk for congenital anomaly. Alcohol is [a] carcinogen, so excessive drinking causes liver cancer, gastric adenocarcinoma and so on.”
-
“Drinking during pregnancy, underage drinking, and excessive drinking cause congenital anomaly, brain development disruptions and cancer, respectively.”
-
“Drinking during pregnancy increases the risk for congenital anomaly, Excessive drinking causes stroke, memory loss and dementia.
The previous warning labels, stemming for 1995, did not all refer to the dangers of drinking while pregnant, and focused on liver conditions only.
There are specific requirements for the design and placement of the warning sentence. The text is supposed to be printed in at least one-tenth of the size of the brand label, and in at least 7-point font size for containers with less than 300 ml, or at least 9-point font size on containers with more than 300 ml. In addition, there are colour and placement requirements to ensure the label is easily seen.
However, a review by the Korea Public Health Association showed that, in 2014, the warning sentences on 81 out of 100 products did not follow the design guidelines (Hani.co.kr, 2016[42]). For example, 55 products used colours that were not distinctive enough from the rest of the label, 56 placed the warning at the bottom of the label, and 34 breeched the minimum font size regulation. Nevertheless, there is little the Ministry can do to enforce the design requirements. While there is a penalty clause in the National Health Promotion Act for not including the warning sentence, there is not one for violating the design requirements.
The rise in ready-to-drink and flavoured alcohol products has lead the Ministry of Food and Drug Safety to introduce mandatory labelling of non-alcoholic sparkling and mixed drinks to indicate that they do not contain alcohol. This policy is aimed at young consumers to educate them and prevent the formation of bad habits (Ministry of Food and Drug Safety, 2017[43]).
2.2.6. Sales and consumption regulations
While restricting the sale and use of alcohol in public places is being considered by the Ministry of Health as well as local governments, so far there are very few regulations on alcohol sales and use. Alcohol can be sold anywhere and at any time – the only exceptions are sales to underage people and online sales. For the latter, an exception is made for designated traditional liquors, to promote their sale and export.
To sell alcohol in Korea, vendors need to apply for an alcohol license (Statutes of the Republic of Korea, 2009[23]). However, contrary to some other OECD countries, this licensing system is not used to limit the density of alcohol vendors or their location (World Health Organization, 2014[44]; OECD, 2015[45]). Supermarkets are the most common place to buy alcohol during the daytime, but late at night and in the early morning, people use liquor shops and small grocery stores more often. (Amista, Chun and Yun, 2017[46]).
Local initiatives have been explored to create alcohol-free zones. In 2017, Seoul City passed an ordinance which designated 22 parks as alcohol free, effective from the 1st January 2018, setting a fine of KWN 100 000 for violations of the ban. However, enforcement of this regulation is not possible as there is no legal basis to support it in National Health Promotion Act. Instead, fines can be written for excessive drinking as a form of disorderly behaviour, but this is difficult to define and enact. The Ministry of Health is working on changing the National Health Promotion Act to allow local governments to implement and enforce alcohol bans (Korea Times, 2018[47]).
In Korea, there are high rates of harmful alcohol use in college students (Kim and Park, 2015[13]). To address this issue, the Ministries of Health and of Education are working with universities to reduce the availability and consumption of alcohol on campuses.
Initiation and orientation activities for new students at universities at the beginning of the school year have repeatedly resulted in deaths from alcohol use (Ministry of Health and Welfare, 2011[48]). In 2011, the Ministry of Education, Science and Technology, the Ministry of Health and Welfare, the Korea University Education Council and the Korea College of Education worked together to develop practice guidelines to reduce harmful drinking in new students. The guidelines focus on education, limiting alcohol advertising on campus, and creating alcohol-free zones in dormitories, classrooms, student assembly halls and student lounges (Korea Times, 2017[49]; Ministry of Health and Welfare, 2011[48]).
In 2018, the Ministry of Education and National Tax Service announced that student bodies were not licensed to sell alcohol in student-run pop-up bars during the popular end-of-year festivals that take place in the spring. This move was met with strong criticism. The notice was issued days before some festivals were about to start, giving organisers little time to adjust, and without adequate consultation. Moreover, the festivals and the pop-up bars were considered a tradition. In practice the ban appeared to have had little impact on alcohol consumption and binge drinking, as students still could buy alcohol from nearby retailers (The Korea Times, 2018[50]).
2.2.7. Treatment of alcoholism and prevention of relapse
There are seven designated, specialist hospitals in Korea that offer inpatient treatment for alcoholism and alcohol-associated disease treatment, all of which are public. They generally offer 8 to 12 week intensive programmes. In 2017, 46 thousand patients received inpatient care, and 77 thousand received outpatient care. Nevertheless, inpatient treatment accounts for almost all of the expenditure on alcohol use disorders, with only 5.8% of the KRW 352 billion going to outpatient care in 2017.
In the community, Addiction Management Centers provide addiction case management and counselling services for alcoholism. Brief interventions, consisting of 3 to 4 counselling sessions combined with physiological test, are offered, after which patients can be registered for long-term care according to an Individualised Service Plan (ISP). The ISP can last as long as needed, and is tailored to the patient’s level of motivation.
Treatment of alcoholism is hampered by limited integration between detection, inpatient and outpatient services (Kim et al., 2013[21]). There are examples of local Addiction Management Centers attempting to solve these issues. Through outreach programmes in the community they aim to identify patients at risk and provide them with timely interventions. To increase the number of patients receiving outpatient counselling after their discharge, counsellors from the Addiction Centers visit inpatient wards to establish contact. However, these practices are not regulated or funded.
Another issue is the lack of funding for treatment and counselling. Addiction Management Centers are dependent on the central, prefectural and municipal government for their budget, and the budget therefore varies depending on the interest and commitment of these bodies. Most Centers cover a large catchment area (e.g. 4 treatment Centers, with 4 to 8 staff members each, cover the entire Seoul population of nearly 10 million), and also deal with other addiction problems such as drugs, internet and gambling (see Box 2.3). As a result, many of the alcohol outreach programmes are restricted to the district in which the clinic is located.
Outpatient treatment for alcohol addiction in Korea takes place in Addiction Management Centers, which also treat a range of other addictions, including drugs, internet and gambling. While this means that the Centers face an increased workload, it also provides benefits, as many patients have more than one addiction.
While the link between gambling or drug addiction and alcohol addiction is widely acknowledged, internet addiction is a relatively new concept. Nevertheless, a relation between this addiction and alcohol use has been observed. Especially in adolescents and young adults, internet addiction often presents alongside alcohol addiction in Korea (Park et al., 2017[51]; Lee et al., 2013[52]). The symptoms observed for both conditions are comparable: changes in cerebral function, lying, difficulty with stopping the addictive behaviour, irritation and anger, difficulty in maintaining study or other everyday functions, and the occurrence of health problems (Kim et al., 2006[53]). Research has found that people with alcohol addiction and with internet addiction are similar terms of emotion, temperament, and personality traits (Hwang et al., 2014[54]). This close relation between the two addictions suggests that treatment responses could also be related.
Source: Park, S. et al. (2017[51]) “Prevalence and Psychiatric Comorbidities of Internet Addiction in a Nationwide Sample of Korean Adults.”, Psychiatry investigation, Vol. 14/6, pp. 879-882, https://doi.org/10.4306/pi.2017.14.6.879; Lee, Y. et al. (2013[52]), “Substance abuse precedes Internet addiction.”, Addictive behaviors, Vol. 38/4, pp. 2022-5, https://doi.org/10.1016/j.addbeh.2012.12.024; Kim, K. et al. (2006[53]), “Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: A questionnaire survey”, International Journal of Nursing Studies, Vol. 43/2, pp. 185-192, https://doi.org/10.1016/J.IJNURSTU.2005.02.005; Hwang, J. et al. (2014[54]), “Shared psychological characteristics that are linked to aggression between patients with Internet addiction and those with alcohol dependence”, Annals of General Psychiatry, Vol. 13/1, p. 6, https://doi.org/10.1186/1744-859X-13-6.
2.2.8. Drink-driving
As described earlier, drink-driving is a major issue in Korea, where the rate of alcohol-related road traffic crashes is one of the highest among OECD countries. While up until recently the national maximum legal blood alcohol concentration for drivers was 0.05% (in line with many other OECD countries, see Figure 2.14), from June 2019 it was lowered to 0.03%. These reforms follow the changes made in Japan (see Box 2.4).
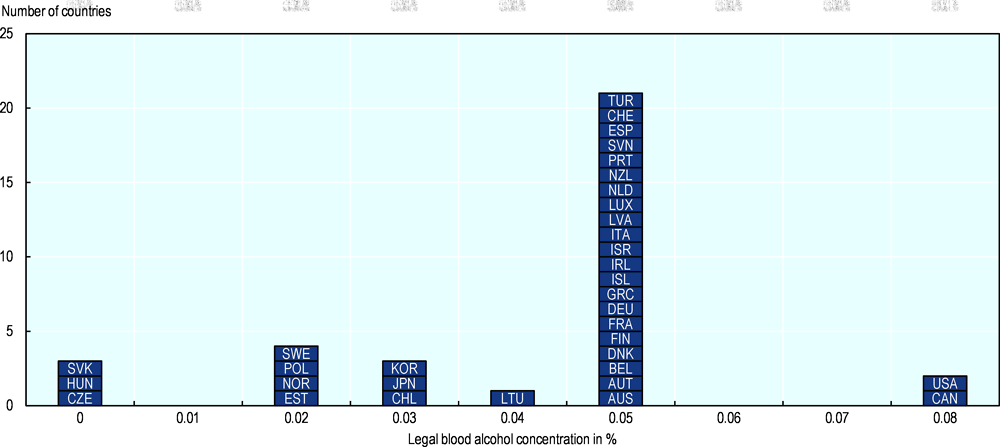
Source: World Health Organization (2018[3]), Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en.
In 2002, Japan lowered the legal blood alcohol concentration limit from 0.05% to 0.03% (OECD, 2015[45]). In addition, the penalties for drink-driving were increased: the fine for driving while intoxicated was increased from JPY 50 000 to 500 000, amongst other measures.
The measures appear to have been successful. One study, comparing motor vehicle crash rate due to alcohol per 100 000 licensed drivers before (1998-2001) and after (2002-2005) the introduction of the new regulation, found that the number of crashes among 16-19 year olds, adult males and adult females decreased by 64%, 50% and 52%, respectively (Desapriya et al., 2007[55]). Another study found that alcohol-related traffic fatalities per billion kilometres driven decreased by 38% in the post-law period, and alcohol-related traffic injuries by 33% (Nagata et al., 2008[56]). However, others have suggested that these decreases were also due to the news coverage of a high-profile fatal crash in November 1999 (Nakahara, Katanoda and Ichikawa, 2013[57]).
Source: OECD (2015[45]), Tackling Harmful Alcohol Use: Economics and Public Health Policy, OECD Publishing; Desapriya, E. et al. (2007[55]), “Impact of lowering the legal blood alcohol concentration limit to 0.03 on male, female and teenage drivers involved alcohol-related crashes in Japan”, International Journal of Injury Control and Safety Promotion, Vol. 14/3, pp. 181-187, https://doi.org/10.1080/17457300701440634; Nagata, T. et al. (2008[56]), “Effectiveness of a law to reduce alcohol-impaired driving in Japan.”, Injury prevention : journal of the International Society for Child and Adolescent Injury Prevention, Vol. 14/1, pp. 19-23, https://doi.org/10.1136/ip.2007.015719; Nakahara, S., K. Katanoda and M. Ichikawa (2013[57]), “Onset of a declining trend in fatal motor vehicle crashes involving drunk-driving in Japan.”, Journal of epidemiology, Vol. 23/3, pp. 195-204, https://doi.org/10.2188/JEA.JE20120134.
In 2011, the fines for drink-driving were revised, differentiating them based on the blood alcohol level at the time of the offense (Jeju Weekly, 2011[58]; Statutes of the Republic of Korea, 2012[59]) (see Table 2.2). With the new drink-driving limit introduced in 2019, the penalties were adjusted again – becoming much tougher.
In addition, a new provision prohibiting riding bicycles while intoxicated took effect in September 2018. Anyone who rides a bicycle while over the legal alcohol limit is subject to a fine of up to KRW 200 000, or detention.
copy the linklink copied!2.3. To reduce harmful alcohol use, Korea should implement a range of alcohol policies
The Korean government recognises the issues that exist around harmful alcohol use, and has stepped up its public health response. A number of new policies have been implemented, and while the design may be optimised in some cases (for example the warning labels on containers), these new policies bring Korea closer to OECD best practice (for example the drink-driving limits). In other cases, there is the motivation to make changes – to regulate advertising or public drinking– but it remains a struggle to get these policies implemented.
One of the main factors preventing the implementation of more comprehensive prevention policies is the social acceptability of alcohol in Korea (Seo et al., 2015[60]). Alcohol plays a central and important part in Korean daily life, and public and professionals alike are opposed to restrictive policies. It is therefore crucial to design new policies by taking into account this cultural factor. Implementing a wide range of policies, part of the WHO global strategy to reduce the harmful use of alcohol (World Health Organization, 2010[61]), can help to de-normalise harmful drinking and change the public acceptability and desirability of harmful drinking. Global action to tackle tobacco smoking suggests that comprehensive policy packages may be successful in decreasing the social acceptability of unhealthy lifestyles (see Box 2.5).
Ever since the negative health impacts of tobacco became apparent, public health agencies and governments have worked to reduce smoking. In the last decade, significant process has been made in OECD countries, reducing the proportion of daily smokers from 24% in 2005 to 18% in 2015 (OECD, 2017[62]). These reductions are the result of several different policies, including taxation, bans on smoking in public places, mass media campaigns, support for people who want to quit, advertising restriction and warning labels on packages.
While each of these policies has had a direct influence on tobacco use, together they have also brought about a shift in public opinion regarding smoking. Research has shown that the interventions with the greatest impact on tobacco use are those that alter the social contexts and incentives (Cummings and Proctor, 2014[63]). Smoking bans in public places have been shown to reduce the perceived social acceptability of smoking (Albers et al., 2004[64]; Thrasher et al., 2009[65]), and are associated with an increase in homes that are kept smoke-free (Nyborg and Rege, 2003[66]). Awareness of anti-tobacco information and smoking restrictions has been found to be associated with feeling uncomfortable about smoking and societal disproval of smoking (Rennen et al., 2014[67]).
Existing policies can also contribute to the acceptability of additional regulations. Exposure to anti-tobacco campaigns has been shown to be correlated with a favourable attitude towards new potential tobacco regulations (Schmidt et al., 2018[68]). Other studies have found that support for smoking bans increased after they were implemented in Scotland (Brown, Moodie and Hastings, 2009[69]), Mexico (Thrasher et al., 2010[70]), the United Kingdom, France, Germany and the Netherlands (Mons et al., 2012[71]), because of their impact on social norms.
Finally, the sequenced implementation of a wide range of policies focused at smoking can support the psychological perception of a major change, and further contribute to a change in the social norm (Nyborg et al., 2016[72]).
Sources: OECD (2017[62]), Health at a Glance 2017: OECD Indicators, OECD Publishing, Paris, https://doi.org/10.1787/health_glance-2017-en; Cummings, K. and R. Proctor (2014[63]), “The changing public image of smoking in the United States: 1964-2014.”, Cancer Epidemiol Biomarkers Prev, Vol. 23/1, pp. 32-6, https://doi.org/10.1158/1055-9965.EPI-13-0798; Albers, A. et al. (2004[64]) , “Relation between local restaurant smoking regulations and attitudes towards the prevalence and social acceptability of smoking: a study of youths and adults who eat out predominantly at restaurants in their town”, Tobacco Control, Vol. 13, pp. 347-355, https://doi.org/10.1136/tc.2003.007336; Thrasher, J. et al. (2009[65]), “Smoke-free policies and the social acceptability of smoking in Uruguay and Mexico: findings from the International Tobacco Control Policy Evaluation Project.”, Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco, Vol. 11/6, pp. 591-9, https://doi.org/10.1093/ntr/ntp039; Nyborg, K. and M. Rege (2003[66]), “On social norms: the evolution of considerate smoking behavior”, Journal of Economic Behavior & Organization, Vol. 52/3, pp. 323-340, https://doi.org/10.1016/S0167-2681(03)00031-3; Rennen, E. et al. (2014[67]), “Associations between tobacco control policy awareness, social acceptability of smoking and smoking cessation. Findings from the International Tobacco Control (ITC) Europe Surveys”, Health Education Research, Vol. 29/1, pp. 72-82, https://doi.org/10.1093/her/cyt073; Schmidt, A. et al. (2018[68]), “Attitudes towards Potential New Tobacco Control Regulations among U.S. Adults”, Int. J. Environ. Res. Public Health, Vol. 15/72, https://doi.org/doi:10.3390/ijerph15010072; Brown, A., C. Moodie and G. Hastings (2009[69]), “A longitudinal study of policy effect (smoke-free legislation) on smoking norms: ITC Scotland/United Kingdom”, Nicotine & Tobacco Research, Vol. 11/8, pp. 924-932, https://doi.org/10.1093/ntr/ntp087; Thrasher, J. et al. (2010[70]), “Differential impact of local and federal smoke-free legislation in Mexico: a longitudinal study among adult smokers”, Salud Pública de México, Vol. 52, pp. S244-S253, https://doi.org/10.1590/S0036-36342010000800020; Mons, U. et al. (2012[71]), “Comprehensive smoke-free policies attract more support from smokers in Europe than partial policies”, The European Journal of Public Health, Vol. 22/suppl 1, pp. 10-16, https://doi.org/10.1093/eurpub/ckr202; Nyborg, K. et al. (2016[72]), “Social norms as solutions”, Science, Vol. 354/6308, pp. 42-43, http://science.sciencemag.org/content/354/6308/42.
Korea should consider implementing a comprehensive policy package to tackle harmful alcohol consumption that acts at different levels (Lee, 2019[73]). Actions to reduce the impact of advertising and to regulate the availability of alcohol can help reduce constant exposure to marketing and prevent easy access to alcohol, particularly for vulnerable and high-risk groups. Education interventions can increase awareness, help people manage social pressure and, if well designed, can help mobilise public opinion and support for effective alcohol policies. Finally, price policies can act as a barrier to underage drinking or reduce harmful consumption.
2.3.1. Reduce the constant exposure to marketing by regulating advertising and media portrayal
In Korea, regulation of alcohol advertising is more limited than in many other OECD countries. Advertisements can be seen on street corners and public transport, television programmes feature young people engaging in heavy drinking with friends (The Korea Herald, 2017[38]), and K-Pop celebrities promote soju on billboards and TV (European Centre for Monitoring Alcohol Marketing, 2019[37]). This leads to a constant exposure to alcohol advertisement.
One strategy to reduce the exposure to alcohol publicity is to regulate advertising and other marketing. Currently Korea has some restrictions on television advertising, but other media remain available to alcohol marketing. Many OECD countries have considerably restricted the advertisement of alcohol (OECD, 2015[45]). In France, the Loi Évin prohibits the advertising of all alcoholic beverages containing over 1.2% ABV on television and in cinemas, as well as sponsorship of sports or cultural events, and restricts marketing on the internet (an exception to these restrictions is advertisement of oenological information and promotion of a certain region or terroir). In Norway, any form of mass communication on alcohol is prohibited, including advertisements in printed newspapers, films, radio, television, telephone networks, data networks, illuminated advertisement hoardings, signboards and similar devices, depictions and exhibitions.
Comprehensive bans are the most effective in reducing exposure to alcohol use, as partial bans can lead to a displacement rather than a reduction in marketing (World Health Organization, 2011[74]; OECD, 2015[45]). Korea should therefore aim to implement comprehensive regulations on alcohol advertisement and other marketing. However, implementing a complete ban may not be feasible right away, both due to the political climate in Korea and the complexity of designing and enforcing such regulation, in particular regarding internet and social media advertising (OECD, 2015[45]). As a first step towards comprehensive regulations, Korea could consider addressing print, television and outdoor advertising. This would considerably reduce the public’s exposure to alcohol marketing, and the restrictions could be further expanded once the acceptability of such regulation increases. Regulations in other countries can provide a blueprint to expand marketing restrictions to platforms such as social media and the internet (see Box 2.6).
In 2015, Finland was the first country in the world to introduce regulation on the use of social media for the purpose of marketing alcohol products. The Finnish Alcohol Act prohibits the use of user-generated or user-shared content. The National Supervisory Authority for Welfare and Health (Valvira) is responsible for the implementation and enforcement of marketing regulations in Finland. Valvira has set out guidelines that interpret the social media restrictions for alcohol producers, stating that they cannot:
-
Use or distribute content generated by consumers, such as comments or pictures of alcoholic products, for advertising.
-
Provide a sharing function when advertising alcoholic beverages, or encourage consumers to share content.
However, execution and enforcement of social media marketing regulations is complicated. In some cases, it might not be possible to disable a sharing function on a third-party social media platform. When it comes to enforcement, it can be difficult to identify marketing by alcohol companies when this is done through influencer marketing and other advanced product placement techniques. While the Finish regulations have been formulated to apply even in the case of advertising distributed through another country, the global nature of social media and the internet make national laws hard to enforce.
Source: Kauppila, E. et al. (2019[75]), Alcohol Marketing on Social Media Sites in Finland and Sweden, Faculty of Social Sciences, University of Helsinki, https://blogs.helsinki.fi/hu-ceacg/files/2019/04/Alcohol-marketing-on-social-media-sites-in-Finland-and-Sweden-2019.pdf (accessed on 20 January 2020).
In addition to regulating the media channels used for advertising, Korea should also review which content is allowed. The depiction of adolescents and pregnant women is not permitted, but otherwise the messaging is unrestricted. The use of widely popular K-Pop artists in advertisements, or the depiction of drinking in television shows with attractive actors and in social situations, can make drinking seem desirable. Moreover, it appeals to younger audiences in particular, who are particularly susceptible to advertising (OECD, 2015[45]).
To address this powerful exposure, it is important that Korea redouble its efforts to implement regulation that controls these types of marketing. The recent proposal to ban the use of models and celebrities is a positive first step, but – if implemented – this would not limit the messaging of advertisements. Instead, more wide-ranging regulations should be considered, to ban the association of alcohol with popularity, beauty and success.
An example of such regulation is the Loi Évin in France, which limits the content of alcohol advertisements to ‘objective’ characteristics of the product (e.g. alcohol content, origin, means of production) (OECD, 2015[45]). In New Zealand, the Code for Advertising and Promotion of Alcohol states that alcohol advertisements cannot promote drinking alcohol as a better or more attractive lifestyle choice; imply that the success of a social occasion depends of alcohol; suggest that alcohol can lead to sexual, social, sporting or business success or popularity; or is necessary to achieve social status with peers (Advertising Standards Authority, 2017[76]).
In addition to regulating the marketing of alcohol products, Korea should also consider regulating the portrayal of alcohol use in regular media. While content for audiences over the age of 19 can only be show at certain times, many television dramas that depict alcohol are rated appropriate for audiences 15 years and older, and can therefore be shown at any time. Other countries have implemented graded restrictions: in Finland, content for audiences over 16 cannot be shown before 9pm, and for audiences over 18 before 11pm; in Germany content for over 16 year olds can be shown at 10pm, and for over 18 year olds at 11pm. Korea could consider implementing a similar regulation on content for audiences over 15 years old, to reduce their exposure to glamorised and socialised drinking in television shows.
2.3.2. Control the availability of alcohol by regulating sales and consumption
Currently, there are limited regulations on where alcohol can be bought and consumed. The wide availability of alcohol can increase consumption, and create a perception of social acceptance of drinking, particularly in adolescents (Paschall, Lipperman-Kreda and Grube, 2014[77]). Alcohol availability restrictions have been proven to be effective in reducing the general level of harmful use of alcohol. (OECD, 2015[45]). Korea could consider regulation to restrict the places at which alcohol can be bought, the times during which it can be bought, as well as the places it can be consumed.
The existing licensing system in Korea could be used to regulate the density of alcohol vendors, to decrease alcohol use. Two systematic reviews have found that the density of alcohol outlets was associated with an increase in alcohol consumption (Popova et al., 2009[78]; Bryden et al., 2012[79]). In Scotland for example, the licensing board must refuse an application for a new license if this would result in the overprovision of licensed premises in the locality (Scottish Government, 2005[80]).
In addition to controlling the density of alcohol vendors, Korea could also consider regulating alcohol sales at petrol stations and other highway establishments. In 2010, Italy expanded its regulation of the sales of alcohol at petrol stations and motorway service stations: no spirits can be sold there between 10pm and 6pm, and no alcohol at all between 2am and 6am (OECD, 2015[45]). In the two subsequent years, highway accidents involving an injury or death decreased by 15.3% and 14% respectively. Considering the high rate of alcohol-related accidents in Korea, this could make a considerable impact.
Korea could also implement regulations on the time at which alcohol is available for sale and consumption. There is evidence that controlling alcohol sales hours can reduce alcohol-related injuries, homicides and other crime (Sanchez-Ramirez and Voaklander, 2017[81]), in particular when restricting evening opening hours for on-premise trade, including bars and clubs (Hahn et al., 2010[82]; Wilkinson, Livingston and Room, 2016[83]). However, the sale of alcohol can also be limited at other times. For example, New York prohibits bars and restaurants from selling alcohol before 10am on Sundays.
Finally, Korea could consider legislation to support local governments in their attempt to restrict alcohol consumption in certain public spaces. Local governments in Korea are already implementing alcohol-free zones in parks, but they currently lack the legal basis to enforce these laws. The National Health Promotion Act does not give local governments the right to enforce public drinking bans. In the case of tobacco, the National Health Promotion Act does includes a clause that allows local governments to designate and enforce smoke-free zones, which sets a legal precedent to include similar provisions for alcohol.
Once the appropriate laws are in place, municipalities should be encouraged to review their local environment for places where alcohol consumption should be restricted and implement such measures (see Box 2.7).
Several OECD countries have given local governments the power to introduce alcohol-free zones, which function in addition to nation-wide regulation of drinking in public institutions such as hospitals and schools. This approach empowers municipalities to introduce bans where they are most needed or most effective.
In the Australian state of New South Wales, local governments have the legislative power to establish alcohol-free zones or alcohol-prohibited areas. Within these zones, police officers are allowed to confiscate open alcohol containers and impose fines of up to AUD 2 200 (KRW 1 750 000). Over 80% of the 152 local government authorities have implemented such zones (Fisher, Wadds and Clancey, 2018[84]), which include car parks, streets, beaches, playgrounds, reserves, sporting fields and parks.
In the Netherlands, mayors hold the power to introduce “Algemene Plaatselijke Verordeningen” (General local ordinances, or APVs). These APVs can restrict alcohol consumption in certain areas or streets, or at certain times (for example on match days around sport stadiums). Decentralising this decision making to the local governments allows policies to be tailored to local circumstances. For example, in the municipality of The Hague, the local government reviews the area’s crime statistics every year to identify where the alcohol-bans should apply (Gemeente Den Haag, 2017[85]). Perpetrators can be given monetary fines.
In Sweden, the municipalities are responsible for a large number of alcohol policies, including licensing, public education and rehabilitation (Karlsson, 2012[86]). In addition to these obligatory duties, the municipalities have the freedom to implement other alcohol regulations, including local restrictions on the consumption of alcohol in public places.
Sources: Fisher, D., P. Wadds and G. Clancey (2018[84]), “The patchwork of alcohol-free zones and alcohol-prohibited areas in New South Wales (Australia)”, Safer Communities, Vol. 17/2, pp. 94-102, https://doi.org/10.1108/SC-06-2017-0025; Gemeente Den Haag (2017[85]), Alcohol-gebiedsverbod, https://www.denhaag.nl/nl/in-de-stad/veiligheid/alcohol-gebiedsverbod.htm (accessed on 19 November 2018); Karlsson, D. (2012[86]), “Alcohol policy and local democracy in Sweden”, Nordic Studies on Alcohol and Drugs, Vol. 29/3, pp. 233-252, https://doi.org/10.2478/v10199-012-0016-9.
2.3.3. Invest in education to increase awareness, reduce social pressures and to mobilise public opinion
Existing information campaigns have focused on providing tools to resist social pressures and reduce consumption, by giving explicit instructions on how to consume alcohol safely and how to say no. For university students, the Ministry has developed and disseminated a Moderate Drinking Code and set up a programme to train and assist moderate drinking supporters.
Korea should consider setting up similar dedicated educational programmes for other high-risk groups: school students and employees.
Early education in a school-based setting should aim to delay the initiation of drinking and prevent the establishment of harmful drinking habits. The Ministry of Health has indicated that it is looking to expand alcohol education in schools. While evidence of the effectiveness of school-based alcohol education programmes is relatively weak, programmes centred on enhancing basic skills such as critical thinking and resistance to social influences show promise (OECD, 2015[45]). Research has shown that effective school-based interventions need to address social norms around alcohol use and build personal and social skills to help resist pressure to use alcohol (Stigler, Neusel and Perry, 2011[87]) (see Box 2.8).
The past two decades have seen a rapid spread of life skills education programmes, encouraged by international organisations such as the WHO and UNICEF, and implemented in national policies by many countries (UNICEF, 2012[88]). Life skills education aims to provide people with knowledge and skills to protect them from harm or abuse (Nasheeda et al., 2018[89]). Such skills include communication, assertiveness, self-awareness, decision-making, and critical thinking.
Many school-based life skill education programmes focus on specific life skills, such as dealing with smoking, alcohol and drug use, and sexual activities (Nasheeda et al., 2018[89]). In this case, life skills education aims to provide students with a critical understanding of the health impact of their choices, and with negotiation or refusal skills to manage peer pressure.
There is some evidence that life skill education programmes reduce the frequency of alcohol consumption and episodes of drunkenness among school-aged children, though studies are often subject to methodological limitations (Martin, Nelson and Lynch, 2013[90]). A study looking at the long-term impact of a life skills programme on substance use in Germany found that the students who received the intervention showed less increase in alcohol consumption over the first three years – during which they received booster sessions after the initial programme – but caught up to the control group after this (Weichold and Blumenthal, 2016[91]). The researchers suggest that further booster sessions may be needed once alcohol use becomes highly normative among peers.
Sources: UNICEF (2012[88]), Global evaluation of life skills education programmes, UNICEF, New York, https://www.unicef.org/evaldatabase/files/UNICEF_GLS_Web.pdf (accessed on 13 August 2018); Nasheeda, A. et al. (2018[89]), “A narrative systematic review of life skills education: effectiveness, research gaps and priorities”, International Journal of Adolescence and Youth, pp. 1-18, https://doi.org/10.1080/02673843.2018.1479278; Martin, K., J. Nelson and S. Lynch (2013[90]), Effectiveness of school-based life-skills and alcohol education programmes: a review of the literature, NFER, Slough, http://www.nfer.ac.uk (accessed on 13 August 2018); Weichold, K. and A. Blumenthal (2016[91]), “Long-Term Effects of the Life Skills Program IPSY on Substance Use: Results of a 4.5-Year Longitudinal Study”, Prevention Science, Vol. 17/1, pp. 13-23, https://doi.org/10.1007/s11121-015-0576-5.
Similar skills are needed in the workplace, where drinking is an important part of the social environment. After-hour company dinners, also known as hoesnik or hweshik, frequently involve large amounts of alcohol (Çakar and Kim, 2016[92]). Employees can experience social pressure to participate due to the hierarchical nature of work teams, the etiquettes around drinking and dining, and the bonding aspect associated with social drinking, which can translate into job progression.
Employers can consider implementing an alcohol code of conduct (Work Safe Victoria, 2017[93]). While such codes are more difficult to enforce outside of the workplace, employers can promote recommendations such as the “119” plan. These types of guidelines, which recommend reducing the alcohol intake and ending the night earlier, can be particularly helpful for hweshik, which often involve bar hopping until late in the evening on a weekday. These guidelines should be targeted in particular at managers or other high-ranking supervisors, as they are often the decision makers at these events. As companies and local governments are starting to experiment with these guidelines, it would be interesting to evaluate their impact and effectiveness.
In addition to codes of conduction, companies should be encouraged to set-up workplace-based alcohol prevention programmes. These programmes can include education (using written communication, face-to-face conversations or presentations, or web-based counselling), peer-based interventions or employee assistance programmes for those with dependency (see Box 2.9).
Web-based interventions: A Cochrane review of programmes that provide personalised alcohol consumption advice via computer or mobile devices found that it could help people reduce heavy drinking – reducing alcohol consumption by of up to three (UK) standard drinks per week on average (Kaner et al., 2017[94]). Such interventions have the benefit that they can be conducted in private by the employee, avoiding any stigma (Khadjesari et al., 2014[95]). An interactive online intervention can also be personalised and may be delivered at a low cost and a convenient time.
Peer-based interventions: Some employers have implemented peer-based interventions to reduce alcohol-related harm, which a focus on changing workplace culture, attitudes, and perceptions around alcohol (OECD, 2015[45]). One example is the Team Awareness programme, which aimed to change the culture by reviewing group risks, promoting responsiveness to problems, and encouraging alternatives to the social bonding provided by drinking. In one experiment, this programme was able to reduce the prevalence of problem drinking from 20% to 11% (Bennett et al., 2004[96]).
Employee Assistance Programmes (EAP): EAPs are common in larger enterprises and can be required by company policy (OECD, 2015[45]). While the core component of EAPs is psychological counselling, programmes can also provide other services such as identification and assessment; mediation; assistance in finding other treatment; and return to work support. A systematic review found that EAPs enhance employee outcomes, in terms of presenteeism and functioning (Joseph, Walker and Fuller-Tyszkiewicz, 2018[97]).
Sources: Kaner, E. et al. (2017[94]), “Does personalised advice via computer or mobile devices reduce heavy drinking?”, Cochrane Database of Systematic Reviews, https://doi.org/10.1002/14651858.CD011479.pub2; Khadjesari, Z. et al. (2014[95]), “Health on the Web: Randomised Controlled Trial of Online Screening and Brief Alcohol Intervention Delivered in a Workplace Setting”, PLoS ONE, Vol. 9/11, p. e112553, https://doi.org/10.1371/journal.pone.0112553; OECD (2015[45]), Tackling Harmful Alcohol Use: Economics and Public Health Policy, OECD Publishing, https://doi.org/10.1787/9789264181069-en; Bennett, J. et al. (2004[96]), “Team awareness, problem drinking, and drinking climate: workplace social health promotion in a policy context.”, American journal of health promotion : AJHP, Vol. 19/2, pp. 103-13, https://doi.org/10.4278/0890-1171-19.2.103; J oseph, B., A. Walker and M. Fuller-Tyszkiewicz (2018[97]), “Evaluating the effectiveness of employee assistance programmes: a systematic review”, European Journal of Work and Organizational Psychology, Vol. 27/1, pp. 1-15, https://doi.org/10.1080/1359432X.2017.1374245.
2.3.4. Review the taxation and pricing policies
Policies to increase the retail price of alcoholic beverages have the potential to generate large health gains (OECD, 2015[45]). While Korea levies excise taxes on alcohol products, they remain relatively cheap. Proposed changes to the tax structure for beer and rice wine are aimed at improving the competitive position of domestic brands but are expected to decrease the tax on domestic beers (The Korea Herald, 2019[24]). Soju in particular is relatively affordable, and as one of the most popular drinks in Korea, this can contribute to the high consumption.
Increasing the price of alcohol is one of the most effective strategies to reduce harmful alcohol use (World Health Organization, 2018[1]). The WHO Global strategy recommends that countries review alcohol prices regularly, looking at inflation and income levels. It also suggests implementing minimum prices where applicable (Box 2.10).
While alcohol taxing has been in use for decennia, minimum pricing is a relatively new policy approach that is gathering interest. The general idea is to charge a minimum price for alcohol products, thus reducing the consumption of low-cost products specifically. In practice, this can be achieved by banning below-cost sales, establishing minimum mark-ups or profit margins, or setting minimum unit prices based on the alcohol content of the beverage (OECD, 2015[45])
Minimum pricing strategies can have certain benefits over taxation. Firstly, because they specifically target very cheap alcohol products, which may be more often purchased by heavy users, they are expected to have more impact on high-risk drinking. Secondly, contrary to taxes, which may not be passed on to the consumer, minimum prices are certain to reach the consumer. On the other hand, while taxes bring in revenue for the government, increased income from minimum prices stays with the producers.
Scotland has become one of the first countries to vote in comprehensive legislation on minimum alcohol prices. With alcohol becoming increasingly affordable, it had become possible to exceed the weekly low risk drinking guidelines of 14 units of alcohol on less than GBP 3 (3.35 EUR) (Scottish Government, 2017[31]). The Alcohol (Minimum Pricing) (Scotland) Act 2012 increased this cost to GBP 7 (7.82 EUR), by setting a minimum price of GBP 0.50 (0.56 EUR) per unit of alcohol, effective 1 May 2018.
An initial evaluation of the minimum price regulation in Scotland, using household shopping panel data, showed an overall GBP 0.064 increase in the price of a gram of alcohol and a reduction of 9.5 grams of alcohol in the weekly per adult per household alcohol purchases. Importantly, this reduction in volume of alcohol purchased only occurred in households that were in the top fifth in terms of alcohol purchasing. For those households, alcohol purchases reduced by 15 g of alcohol per week per adult after the introduction of minimum unit prices (O’Donnell et al., 2019[98]).
Several other countries have implemented, or are considering implementing, similar regulations. Wales has also introduced a GBP 0.50 minimum unit price on alcohol, which will come into force in March 2020 (Wales Statutory Instruments, 2019[99]). Three Canadian provinces have implemented minimum prices in different forms. Quebec’s minimum price regulation applies only to beer and is adjusted based on cost of living (i.e. inflation) (Canadian Association of Liquor Jurisdications, 2013[100]). In British Columbia, minimum prices for alcohol products were introduced in 1989. These do not take into account inflation; however, periodic increases in the floor price are applied (Canadian Association of Liquor Jurisdications, 2013[100]). Saskatchewan requires businesses that serve alcohol to charge a minimum price per ounce of spirits, beer and wine (Stockwell et al., 2012[101]).
Sources: OECD (2015[45]), Tackling Harmful Alcohol Use: Economics and Public Health Policy, OECD Publishing, https://doi.org/10.1787/9789264181069-en; Scottish Government (2017[31]), Minimum Unit Pricing, http://www.gov.scot/Topics/Health/Services/Alcohol/minimum-pricing; O’Donnell, A. et al. (2019[98]), “Immediate impact of minimum unit pricing on alcohol purchases in Scotland: Controlled interrupted time series analysis for 2015-18”, The BMJ, Vol. 366, https://doi.org/10.1136/bmj.l5274; Wales Statutory Instruments (2019[99]), “The Public Health (Minimum Price for Alcohol) (Minimum Unit Price) (Wales) Regulations 2019”.; Canadian Association of Liquor Jurisdications (2013[100]), Minimum Pricing in Canadian Alcohol Jurisdictions; Stockwell et al. (2012[101]), “The raising of minimum alcohol prices in Saskatchewan, Canada: Impacts on consumption and implications for public health”, American Journal of Public Health, http://10.2105/AJPH.2012.301094.
In addition, from a public health perspective, Korea should consider reviewing existing policies that aim to promote the traditional liquor industry. The Act on Promotion of Korean Traditional Liquor Industries notes that while its aim is to promote the competitiveness of tradition liquor industry, it is committed to developing a wholesome drinking culture (Statutes of the Republic of Korea, n.d.[27]). However, aspects of the act could have a negative impact on public health, such as subsidies to people who establish and operate a Center for promotion and exhibition of traditional liquors, or government-operated alcohol fairs. Moreover, the reduced tax rate for traditional liquors – despite applying to only a limited number of producers and a limited volume – can lead to a lower price (Statutes of the Republic of Korea, 2009[23]).
copy the linklink copied!Conclusion
Heavy episodic and high-risk drinking are highly prevalent in the Korean population with a considerable impact on population health and the economy. A number of policies have been implemented to reduce harmful alcohol use, including taxation, drink-driving regulation, and educational programmes in universities. At present, it appears that opposition currently prevents the introduction of a more comprehensive policy package.
There is scope though, to introduce a more comprehensive policy package, and which could well lead to positive outcomes for both population health, and the Korean economy. Korea should focus on changing the culture around harmful drinking, which is currently widely available and a key part of many social events. This would include making it harder to access alcohol, through some regulations on the sale and consumption of alcohol for example not allowing alcohol to be sold in roadside service stations, and examining alcohol pricing policy to better align with public health priorities. Efforts should also be made to reduce the visibility and prevalence of alcohol and imagery related to alcohol in Korean daily life, for example through stricter marketing regulation. Finally, this should be reinforced through education and awareness programmes among all levels of society.
References
[76] Advertising Standards Authority (2017), Code for Advertising and Promotion of Alcohol, http://www.asa.co.nz/codes/codes/code-for-advertising-and-promotion-of-alcohol/ (accessed on 16 August 2017).
[64] Albers, A. et al. (2004), “Relation between local restaurant smoking regulations and attitudes towards the prevalence and social acceptability of smoking: a study of youths and adults who eat out predominantly at restaurants in their town”, Tobacco Control, Vol. 13, pp. 347-355, https://doi.org/10.1136/tc.2003.007336.
[46] Amista, N., S. Chun and M. Yun (2017), “Relationship between Alcohol Purchasing Time and Alcohol Use Disorder in South Korea.”, Osong public health and research perspectives, Vol. 8/6, pp. 405-414, https://doi.org/10.24171/j.phrp.2017.8.6.08.
[32] Angus, C. et al. (2017), Model-based appraisal of the comparative impact of Minimum Unit Pricing and taxation policies in Wales: Interim report Subtitle: An update to the 50p MUP example, Welsh Government, Cardiff, http://gov.wales/statistics-and-research/research-likely-impact-public-attitudes-towards-minimum-unit-price-alcohol/?lang=en (accessed on 22 February 2018).
[96] Bennett, J. et al. (2004), “Team awareness, problem drinking, and drinking climate: workplace social health promotion in a policy context.”, American journal of health promotion : AJHP, Vol. 19/2, pp. 103-13, https://doi.org/10.4278/0890-1171-19.2.103.
[69] Brown, A., C. Moodie and G. Hastings (2009), “A longitudinal study of policy effect (smoke-free legislation) on smoking norms: ITC Scotland/United Kingdom”, Nicotine & Tobacco Research, Vol. 11/8, pp. 924-932, https://doi.org/10.1093/ntr/ntp087.
[79] Bryden, A. et al. (2012), “A systematic review of the influence on alcohol use of community level availability and marketing of alcohol”, Health & Place, Vol. 18/2, pp. 349-357, https://doi.org/10.1016/j.healthplace.2011.11.003.
[92] Çakar, U. and H. Kim (2016), “Korea’s Drinking Culture: When an Organizational Socialization Tool Threatens Workplace Well-being”, Turkish Journal of Business Ethics, Vol. 8/2, pp. 101-121, https://doi.org/10.12711/tjbe.2015.8.0005.
[100] Canadian Association of Liquor Jurisdications (2013), Minimum Pricing in Canadian Alcohol Jurisdictions, https://calj.org/Articles/Publications/ArticleId/42/Minimum-Pricing-in-Canadian-Alcohol-Jurisdictions (accessed on 7 February 2020).
[63] Cummings, K. and R. Proctor (2014), “The changing public image of smoking in the United States: 1964-2014.”, Cancer Epidemiol Biomarkers Prev, Vol. 23/1, pp. 32-6, https://doi.org/10.1158/1055-9965.EPI-13-0798.
[55] Desapriya, E. et al. (2007), “Impact of lowering the legal blood alcohol concentration limit to 0.03 on male, female and teenage drivers involved alcohol-related crashes in Japan”, International Journal of Injury Control and Safety Promotion, Vol. 14/3, pp. 181-187, https://doi.org/10.1080/17457300701440634.
[9] Drinks International (2016), Jinro dominates Millionaires’ Club list again, http://drinksint.com/news/fullstory.php/aid/6248/Jinro_dominates_Millionaires__Club_list_again.html (accessed on 11 July 2018).
[37] European Centre for Monitoring Alcohol Marketing (2019), South Korea puts alcohol ads endorsed by K-pop stars on notice as underage drinking rises, https://eucam.info/2019/12/09/south-korea-puts-alcohol-ads-endorsed-by-k-pop-stars-on-notice-as-underage-drinking-rises/ (accessed on 17 January 2020).
[30] Financial Times (2018), Minimum alcohol price for England back under consideration, https://www.ft.com/content/f2b0adea-52dc-11e8-b3ee-41e0209208ec (accessed on 16 July 2018).
[84] Fisher, D., P. Wadds and G. Clancey (2018), “The patchwork of alcohol-free zones and alcohol-prohibited areas in New South Wales (Australia)”, Safer Communities, Vol. 17/2, pp. 94-102, https://doi.org/10.1108/SC-06-2017-0025.
[16] GBD 2016 Alcohol Collaborators (2018), “Alcohol use and burden for 195 countries and territories, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016”, The Lancet, Vol. 392/10152, pp. 1015-1035, https://doi.org/10.1016/S0140-6736(18)31310-2.
[85] Gemeente Den Haag (2017), Alcohol-gebiedsverbod, https://www.denhaag.nl/nl/in-de-stad/veiligheid/alcohol-gebiedsverbod.htm (accessed on 19 November 2018).
[82] Hahn, R. et al. (2010), “Effectiveness of Policies Restricting Hours of Alcohol Sales in Preventing Excessive Alcohol Consumption and Related Harms”, American Journal of Preventive Medicine, Vol. 39/6, pp. 590-604, https://doi.org/10.1016/j.amepre.2010.09.016.
[42] Hani.co.kr (2016), Hide the warning phrase, http://www.hani.co.kr/arti/society/health/759418.html (accessed on 17 July 2018).
[102] Holmes, J. et al. (2014), “Effects of minimum unit pricing for alcohol on different income and socioeconomic groups: a modelling study”, The Lancet, Vol. 383/9929, pp. 1655-1664, https://doi.org/10.1016/S0140-6736(13)62417-4.
[54] Hwang, J. et al. (2014), “Shared psychological characteristics that are linked to aggression between patients with Internet addiction and those with alcohol dependence”, Annals of General Psychiatry, Vol. 13/1, p. 6, https://doi.org/10.1186/1744-859X-13-6.
[17] Institute for Health Metrics and Evaluation (2017), GBD Compare, https://vizhub.healthdata.org/gbd-compare/ (accessed on 17 January 2020).
[39] Institute of Alcohol Studies (2019), Alcohol and marketing.
[58] Jeju Weekly (2011), Korea cracking down on DWIs, http://www.jejuweekly.com/news/articleView.html?idxno=1793 (accessed on 19 July 2018).
[97] Joseph, B., A. Walker and M. Fuller-Tyszkiewicz (2018), “Evaluating the effectiveness of employee assistance programmes: a systematic review”, European Journal of Work and Organizational Psychology, Vol. 27/1, pp. 1-15, https://doi.org/10.1080/1359432X.2017.1374245.
[12] Jun, H. and S. Chung (2008), “Effects of Workplace Alcohol-related Environment on Drinking Behaviors among Female Employees”, Korean Journal of Health Education and Promotion, Vol. 25/3, pp. 21-43, http://linkinghub.elsevier.com/retrieve/pii/S0306460304000747 (accessed on 12 July 2018).
[94] Kaner, E. et al. (2017), “Does personalised advice via computer or mobile devices reduce heavy drinking?”, Cochrane Database of Systematic Reviews, https://doi.org/10.1002/14651858.CD011479.pub2.
[86] Karlsson, D. (2012), “Alcohol policy and local democracy in Sweden”, Nordic Studies on Alcohol and Drugs, Vol. 29/3, pp. 233-252, https://doi.org/10.2478/v10199-012-0016-9.
[75] Kauppila, E. et al. (2019), Alcohol Marketing on Social Media Sites in Finland and Sweden, Faculty of Social Sciences, University of Helsinki, https://blogs.helsinki.fi/hu-ceacg/files/2019/04/Alcohol-marketing-on-social-media-sites-in-Finland-and-Sweden-2019.pdf (accessed on 20 January 2020).
[7] KCDC (2017), Youth Health Behavior Survey, http://www.cdc.go.kr/CDC/contents/CdcKrContentView.jsp?cid=77749&menuIds=HOME001-MNU1130-MNU2393-MNU2749 (accessed on 18 July 2018).
[95] Khadjesari, Z. et al. (2014), “Health on the Web: Randomised Controlled Trial of Online Screening and Brief Alcohol Intervention Delivered in a Workplace Setting”, PLoS ONE, Vol. 9/11, p. e112553, https://doi.org/10.1371/journal.pone.0112553.
[20] KIHASA (2016), Current status of alcohol and drug addiction and policy responses, https://www.kihasa.re.kr/english/publications/eng_research/view.do?menuId=68&tid=34&bid=30&ano=851 (accessed on 11 July 2018).
[21] Kim, J. et al. (2013), “The current situation of treatment systems for alcoholism in Korea.”, Journal of Korean medical science, Vol. 28/2, pp. 181-9, https://doi.org/10.3346/jkms.2013.28.2.181.
[13] Kim, J. and S. Park (2015), “Association between protective behavioral strategies and problem drinking among college students in the Republic of Korea”, Addictive Behaviors, Vol. 51, pp. 171-176, https://doi.org/10.1016/J.ADDBEH.2015.07.017.
[53] Kim, K. et al. (2006), “Internet addiction in Korean adolescents and its relation to depression and suicidal ideation: A questionnaire survey”, International Journal of Nursing Studies, Vol. 43/2, pp. 185-192, https://doi.org/10.1016/J.IJNURSTU.2005.02.005.
[14] Kim, S., S. Ahn and T. Lim (2015), “Predicting Alcohol Misuse Among College Students in the US and South Korea”, Journal of Ethnicity in Substance Abuse, Vol. 14/3, pp. 308-322, https://doi.org/10.1080/15332640.2014.996313.
[5] Kim, W. and S. Kim (2008), “Women’s Alcohol Use and Alcoholism in Korea”, Substance Use & Misuse, Vol. 43/8-9, pp. 1078-1087, https://doi.org/10.1080/10826080801914212.
[6] KNHANES (2019), Korea National Health and Nutrition Examination Survey, https://knhanes.cdc.go.kr/.
[29] Korea Consumer Agency (2019), Korea Consumer Agency Real Price Information, http://www.price.go.kr (accessed on 28 February 2019).
[34] Korea Expose (2018), Soju Globalization: From Green Bottle to Premium Label, https://www.koreaexpose.com/soju-globalization-high-end-drinking/ (accessed on 16 July 2018).
[36] Korea Health Promotion Institute (2019), Annual expenditure on alcohol advertising, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00691&tableGubun=DATA070201 (accessed on 4 November 2019).
[35] Korea Health Promotion Institute (2019), Annual frequency of alcohol advertising, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00690&tableGubun=DATA070101 (accessed on 4 November 2019).
[41] Korea Health Promotion Institute (2019), National Health Promotion Act Liquor Advertisement Guidebook, https://www.khealth.or.kr/board/view?pageNum=1&rowCnt=10&menuId=MENU00664&maxIndex=99999999999999&minIndex=99999999999999&schType=0&schText=&categoryId=&continent=&country=&upDown=0&boardStyle=&no1=0&linkId=999102 (accessed on 7 February 2020).
[28] Korea Health Promotion Institute (2019), Price Index of mainstream liquor, http://khealth.or.kr/acs/acsStat/result?menuId=MENU00688&tableGubun=DATA040401 (accessed on 4 November 2019).
[22] Korea Health Promotion Institute (2018), Shining youth, challenging leader!, https://www.khealth.or.kr/board/view?pageNum=1&rowCnt=10&menuId=MENU00677&maxIndex=99999999999999&minIndex=99999999999999&schType=0&schText=&categoryId=&continent=&country=&upDown=0&boardStyle=&no1=21&linkId=24886 (accessed on 17 July 2018).
[40] Korea Health Promotion Institute (2017), Drinking environment monitoring, http://www.khealth.or.kr/board/view?linkId=24441&menuId=MENU00646&boardStyle=Gallery (accessed on 13 July 2018).
[33] Korea Herald (2012), Korea counts the cost of cheap alcohol, http://www.koreaherald.com/view.php?ud=20120814001211 (accessed on 16 July 2018).
[18] Korea Institute of Health and Social Affairs (2017), Risks and Socioeconomic Costs of Alcohol-Attributable Illnesses, https://www.kihasa.re.kr/english/publications/eng_research/view.do?menuId=69&tid=34&bid=31&ano=793 (accessed on 9 July 2018).
[25] Korea Times (2019), Korea to switch tax scheme on beer, https://www.koreatimes.co.kr/www/tech/2019/06/694_270088.html (accessed on 20 January 2020).
[47] Korea Times (2018), Gov’t to designate more alcohol-free zones, https://www.koreatimes.co.kr/www/nation/2018/11/119_258845.html (accessed on 19 November 2018).
[49] Korea Times (2017), Alcohol-free campus campaign starts, http://www.koreatimes.co.kr/www/news/nation/2017/03/117_81613.html (accessed on 12 July 2018).
[15] Korea Times (2017), Anger growing against alcohol-influenced crimes, http://www.koreatimes.co.kr/www/nation/2017/12/356_240362.html (accessed on 12 July 2018).
[73] Lee, H. (2019), “Epidemiology of Alcohol Use Disorders and Alcohol Policy”, Journal of Korean Neuropsychiatric Association, Vol. 58/3, p. 152, https://doi.org/10.4306/jknpa.2019.58.3.152.
[52] Lee, Y. et al. (2013), “Substance abuse precedes Internet addiction.”, Addictive behaviors, Vol. 38/4, pp. 2022-5, https://doi.org/10.1016/j.addbeh.2012.12.024.
[90] Martin, K., J. Nelson and S. Lynch (2013), Effectiveness of school-based life-skills and alcohol education programmes: a review of the literature, NFER, Slough, http://www.nfer.ac.uk (accessed on 13 August 2018).
[10] Ministry of Drug and Food Safety (2016), Survey on alcohol consumption.
[43] Ministry of Food and Drug Safety (2017), Notification No 2017-99, http://www.mfds.go.kr/index.do?x=20&searchkey=title:contents&mid=686&searchword=2017-99&y=9&division=&pageNo=1&seq=13562&sitecode=2017-12-06&cmd=v (accessed on 2 July 2018).
[48] Ministry of Health and Welfare (2011), Alcohol-free campus without drinking accidents, http://www.mohw.go.kr/react/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&page=316&CONT_SEQ=249108 (accessed on 17 July 2018).
[71] Mons, U. et al. (2012), “Comprehensive smoke-free policies attract more support from smokers in Europe than partial policies”, The European Journal of Public Health, Vol. 22/suppl 1, pp. 10-16, https://doi.org/10.1093/eurpub/ckr202.
[56] Nagata, T. et al. (2008), “Effectiveness of a law to reduce alcohol-impaired driving in Japan.”, Injury prevention : journal of the International Society for Child and Adolescent Injury Prevention, Vol. 14/1, pp. 19-23, https://doi.org/10.1136/ip.2007.015719.
[57] Nakahara, S., K. Katanoda and M. Ichikawa (2013), “Onset of a declining trend in fatal motor vehicle crashes involving drunk-driving in Japan.”, Journal of epidemiology, Vol. 23/3, pp. 195-204, https://doi.org/10.2188/JEA.JE20120134.
[89] Nasheeda, A. et al. (2018), “A narrative systematic review of life skills education: effectiveness, research gaps and priorities”, International Journal of Adolescence and Youth, pp. 1-18, https://doi.org/10.1080/02673843.2018.1479278.
[72] Nyborg, K. et al. (2016), “Social norms as solutions”, Science, Vol. 354/6308, pp. 42-43, http://science.sciencemag.org/content/354/6308/42.
[66] Nyborg, K. and M. Rege (2003), “On social norms: the evolution of considerate smoking behavior”, Journal of Economic Behavior & Organization, Vol. 52/3, pp. 323-340, https://doi.org/10.1016/S0167-2681(03)00031-3.
[98] O’Donnell, A. et al. (2019), “Immediate impact of minimum unit pricing on alcohol purchases in Scotland: Controlled interrupted time series analysis for 2015-18”, The BMJ, Vol. 366, https://doi.org/10.1136/bmj.l5274.
[4] OECD (2019), OECD Health Statistics 2019, OECD Publishing, Paris, http://stats.oecd.org/.
[62] OECD (2017), Health at a Glance 2017: OECD Indicators, OECD Publishing, Paris, https://doi.org/10.1787/health_glance-2017-en.
[45] OECD (2015), Tackling Harmful Alcohol Use: Economics and Public Health Policy, OECD Publishing, https://doi.org/10.1787/9789264181069-en. (accessed on 26 July 2017).
[51] Park, S. et al. (2017), “Prevalence and Psychiatric Comorbidities of Internet Addiction in a Nationwide Sample of Korean Adults.”, Psychiatry investigation, Vol. 14/6, pp. 879-882, https://doi.org/10.4306/pi.2017.14.6.879.
[77] Paschall, M., S. Lipperman-Kreda and J. Grube (2014), “Effects of the local alcohol environment on adolescents’ drinking behaviors and beliefs”, Addiction, Vol. 109/3, pp. 407-416, https://doi.org/10.1111/add.12397.
[78] Popova, S. et al. (2009), “Hours and Days of Sale and Density of Alcohol Outlets: Impacts on Alcohol Consumption and Damage: A Systematic Review”, Alcohol and Alcoholism, Vol. 44/5, pp. 500-516, https://doi.org/10.1093/alcalc/agp054.
[67] Rennen, E. et al. (2014), “Associations between tobacco control policy awareness, social acceptability of smoking and smoking cessation. Findings from the International Tobacco Control (ITC) Europe Surveys”, Health Education Research, Vol. 29/1, pp. 72-82, https://doi.org/10.1093/her/cyt073.
[81] Sanchez-Ramirez, D. and D. Voaklander (2017), “The impact of policies regulating alcohol trading hours and days on specific alcohol-related harms: a systematic review”, Injury Prevention, pp. injuryprev-2016-042285, https://doi.org/10.1136/injuryprev-2016-042285.
[68] Schmidt, A. et al. (2018), “Attitudes towards Potential New Tobacco Control Regulations among U.S. Adults”, Int. J. Environ. Res. Public Health, Vol. 15/72, https://doi.org/doi:10.3390/ijerph15010072.
[31] Scottish Government (2017), Minimum Unit Pricing, http://www.gov.scot/Topics/Health/Services/Alcohol/minimum-pricing (accessed on 2 August 2017).
[80] Scottish Government (2005), The Overprovision Assessment - Licensing (Scotland) Act 2005, https://www.gov.scot/Publications/2007/04/13093458/5 (accessed on 14 August 2018).
[60] Seo, S. et al. (2015), “Korean public opinion on alcohol control policy: A cross-sectional International Alcohol Control study”, Health policy, Vol. 119, pp. 33-43, https://doi.org/10.1016/j.healthpol.2014.10.016.
[59] Statutes of the Republic of Korea (2012), Road Traffic Act, http://elaw.klri.re.kr/eng_mobile/viewer.do?hseq=22353&type=part&key=11 (accessed on 19 July 2018).
[23] Statutes of the Republic of Korea (2009), Liquor Tax Act, https://elaw.klri.re.kr/kor_service/lawView.do?lang=ENG&hseq=38385 (accessed on 11 June 2018).
[27] Statutes of the Republic of Korea (n.d.), Act on Promotion of Korean Traditional Liquor Industries, http://elaw.klri.re.kr/eng_mobile/viewer.do?hseq=25641&type=new&key= (accessed on 18 June 2018).
[26] Statutes of the Republic of Korea (n.d.), Education Tax Act, https://elaw.klri.re.kr/eng_mobile/ganadaDetail.do?hseq=40921&type=abc&key=EDUCATION%20TAX%20ACT¶m=E (accessed on 16 July 2018).
[87] Stigler, M., E. Neusel and C. Perry (2011), “School-based programs to prevent and reduce alcohol use among youth.”, Alcohol Res Health, Vol. 34/2, pp. 157-62, http://www.ncbi.nlm.nih.gov/pubmed/22330213 (accessed on 13 August 2018).
[101] Stockwell, T. et al. (2012), “The raising of minimum alcohol prices in Saskatchewan, Canada: Impacts on consumption and implications for public health”, American Journal of Public Health, Vol. 102/12, https://doi.org/10.2105/AJPH.2012.301094.
[24] The Korea Herald (2019), Korea to change liquor tax system for first time in 50 years, http://www.koreaherald.com/view.php?ud=20190605000608 (accessed on 20 January 2020).
[38] The Korea Herald (2017), Alcohol flowing freely on Korean TV, http://www.koreaherald.com/view.php?ud=20170905000710 (accessed on 17 January 2020).
[50] The Korea Times (2018), Despite alcohol warnings, students continue festival binge tradition, http://www.koreatimes.co.kr/www/nation/2018/05/113_248826.html (accessed on 3 July 2018).
[65] Thrasher, J. et al. (2009), “Smoke-free policies and the social acceptability of smoking in Uruguay and Mexico: findings from the International Tobacco Control Policy Evaluation Project.”, Nicotine & tobacco research : official journal of the Society for Research on Nicotine and Tobacco, Vol. 11/6, pp. 591-9, https://doi.org/10.1093/ntr/ntp039.
[70] Thrasher, J. et al. (2010), “Differential impact of local and federal smoke-free legislation in Mexico: a longitudinal study among adult smokers”, Salud Pública de México, Vol. 52, pp. S244-S253, https://doi.org/10.1590/S0036-36342010000800020.
[88] UNICEF (2012), Global evaluation of life skills education programmes, UNICEF, New York, https://www.unicef.org/evaldatabase/files/UNICEF_GLS_Web.pdf (accessed on 13 August 2018).
[8] USDA Foreign Agricultural Service (2018), Beer Market Report Korea, https://gain.fas.usda.gov/Recent%20GAIN%20Publications/Beer%20Market%20Report_Seoul%20ATO_Korea%20-%20Republic%20of_2-2-2018.pdf (accessed on 11 July 2018).
[99] Wales Statutory Instruments (2019), “The Public Health (Minimum Price for Alcohol) (Minimum Unit Price) (Wales) Regulations 2019”.
[91] Weichold, K. and A. Blumenthal (2016), “Long-Term Effects of the Life Skills Program IPSY on Substance Use: Results of a 4.5-Year Longitudinal Study”, Prevention Science, Vol. 17/1, pp. 13-23, https://doi.org/10.1007/s11121-015-0576-5.
[83] Wilkinson, C., M. Livingston and R. Room (2016), “Impacts of changes to trading hours of liquor licences on alcohol-related harm: a systematic review 2005–2015”, Public Health Research & Practice, Vol. 26/4, https://doi.org/10.17061/phrp2641644.
[93] Work Safe Victoria (2017), Guide for developing a workplace alcohol and other drugs policy, https://prod.wsvdigital.com.au/sites/default/files/2018-06/ISBN-Guide-for-developing-workplace-alcohol-drugs-policy-2017-03_0.pdf (accessed on 20 November 2018).
[1] World Health Organization (2018), Global status report on alcohol and health 2018, http://apps.who.int/iris/bitstream/handle/10665/274603/9789241565639-eng.pdf?ua=1 (accessed on 24 October 2018).
[3] World Health Organization (2018), WHO Global Information System on Alcohol and Health, http://apps.who.int/gho/data/node.main.GISAH?lang=en (accessed on 19 October 2018).
[19] World Health Organization (2017), Alcohol-related road traffic crashes (%) - by country, Global Health Observatory data repository, http://apps.who.int/gho/data/node.main.A1108?lang=en (accessed on 11 July 2018).
[44] World Health Organization (2014), Alcohol country profiles - Republic of Korea, http://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/kor.pdf (accessed on 19 March 2018).
[11] World Health Organization (2014), Global status report on alcohol and health 2014, http://www.who.int/substance_abuse/publications/global_alcohol_report/msb_gsr_2014_1.pdf?ua=1 (accessed on 24 October 2017).
[74] World Health Organization (2011), Addressing the harmful use of alcohol : a guide to developing effective alcohol legislation, http://www.wpro.who.int/publications/docs/Addressingtheharmfuluseofalcoholforupload.pdf (accessed on 24 October 2017).
[61] World Health Organization (2010), Global strategy to reduce the harmful use of alcohol, http://apps.who.int/iris/bitstream/10665/44395/1/9789241599931_eng.pdf?ua=1&ua=1 (accessed on 26 July 2017).
[2] World Health Organization (n.d.), Alcohol, total per capita (15+ years) consumption (in litres of pure alcohol), https://www.who.int/data/gho/indicator-metadata-registry/imr-details/465 (accessed on 7 February 2020).
Notes
← 1. Fermented liquors - up to 200 ㎘ when producing the liquors less than 500 ㎘ per year; Distilled liquors - up to 100 ㎘ when producing the liquors less than 250 ㎘ per year.
← 2. Using the UK standard of 8g or 10ml of pure alcohol (Holmes et al., 2014[102]).
Metadata, Legal and Rights
https://doi.org/10.1787/be2b7063-en
© OECD 2020
The use of this work, whether digital or print, is governed by the Terms and Conditions to be found at http://www.oecd.org/termsandconditions.
