Mortality from circulatory diseases
Despite substantial declines in recent decades, circulatory diseases remain the main cause of mortality in most OECD countries, accounting for more than one-third (36%) of all deaths in 2015. Prospects for further reductions may be hampered by a rise in certain risk factors such as obesity and diabetes (OECD, 2015). Circulatory diseases cover a range of illnesses related to the circulatory system, particularly ischaemic heart disease (including heart attack) and cerebrovascular diseases such as stroke.
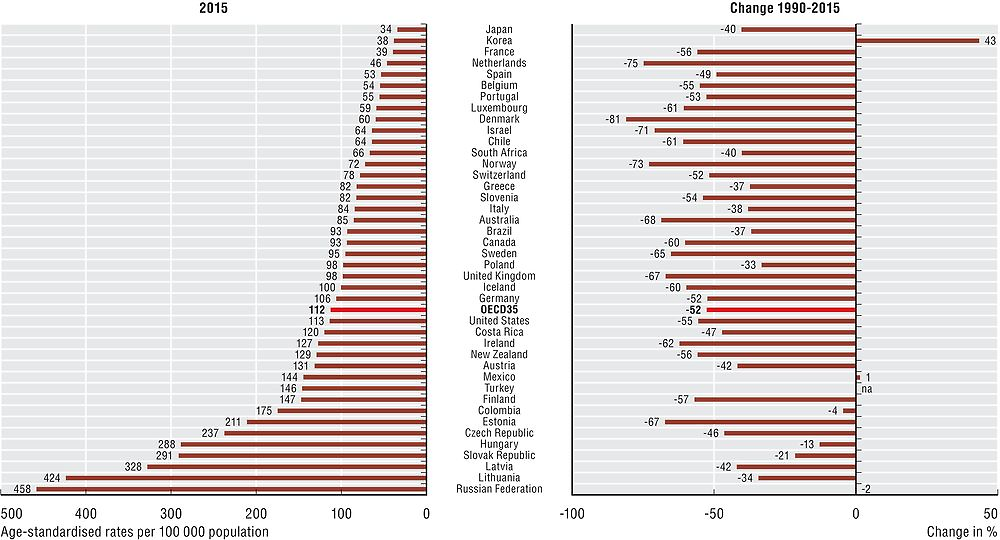
Ischaemic heart disease (IHD) is caused by the accumulation of fatty deposits lining the inner wall of a coronary artery, restricting blood flow to the heart. IHD alone was responsible for nearly 12% of all deaths in OECD countries in 2015. However, mortality from IHD varies considerably across countries (Figure 3.8). Among OECD countries, Central and Eastern European countries report the highest IHD mortality rates. Rates are also high in the Russian Federation. Japan, Korea and France report the lowest rates. Across OECD countries, IHD mortality rates in 2015 were around 82% higher for men than women.
Source: OECD Health Statistics 2017.
IHD mortality rates have declined in nearly all OECD countries, with an average reduction of more than 50% since 1990, contributing greatly to gains in life expectancy, particularly among men. The decline has been most remarkable in Denmark, the Netherlands, Norway and Israel, where rates fell by over 70%. Declining tobacco consumption contributed significantly to reducing the incidence of IHD (see indicator on “Smoking among adults” in Chapter 4), and consequently to reducing mortality rates. Improvements in medical care have also contributed to reduced mortality rates (see indicators on “Mortality following acute myocardial infarction” in Chapter 6 and “Hospital discharges” in Chapter 9).
In Korea, IHD mortality rates have increased substantially since 1990, although they remain low compared with nearly all other OECD countries and have started to fall after peaking in 2006. The initial rise in IHD mortality rates in Korea has been attributed to changes in lifestyle and dietary patterns as well as environmental factors at the time of birth, with people born between 1940 and 1950 facing higher relative risks. In 2006, Korea introduced a Comprehensive Plan to tackle circulatory diseases that encompassed prevention and primary care as well as better acute care, contributing to the reduction in mortality in recent years (OECD, 2012).
Cerebrovascular disease was the underlying cause for about 7% of all deaths in OECD countries in 2015. Cerebrovascular disease refers to a group of diseases that relate to problems with the blood vessels that supply the brain. Common manifestations of cerebrovascular disease include ischaemic stroke, which develops when the brain’s blood supply is blocked or interrupted, and haemorrhagic stroke which occurs when blood leaks from blood vessels into the surface of the brain. In addition to being an important cause of mortality, the disability burden from stroke and other cerebrovascular diseases is also substantial (Feigi et al., 2016).
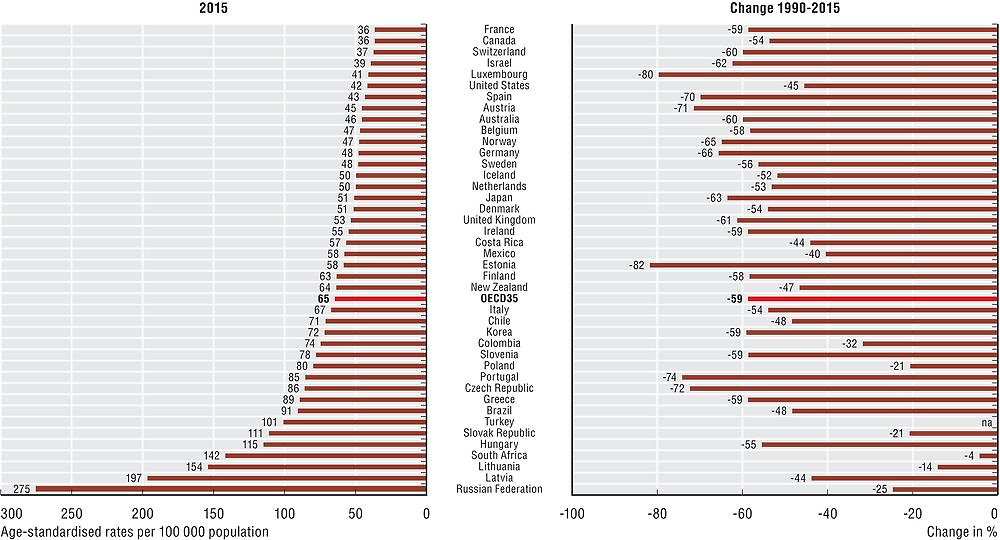
There are large variations in cerebrovascular disease mortality rates across countries (Figure 3.9). Among OECD countries, Latvia, Hungary and the Slovak Republic report a cerebrovascular mortality that is more than three times higher than that of Switzerland, Canada and France, and have the highest mortality rates for both IHD and cerebrovascular disease. Rates are also high in the partner countries of the Russian Federation and South Africa. The high prevalence of risk factors common to both diseases (e.g. smoking and high blood pressure) may explain this link.
Source: OECD Health Statistics 2017.
Since 1990, cerebrovascular disease mortality has decreased in all OECD countries, although to a lesser extent in Poland and the Slovak Republic. On average, the mortality burden from cerebrovascular disease has halved across OECD countries. In Estonia, Luxembourg, Portugal, the Czech Republic and Austria, the rates have been cut by over 70%. As with IHD, the reduction in mortality from cerebrovascular disease can be attributed at least partly to a reduction in risk factors as well as improvements in medical treatments (OECD, 2015; see indicator “Mortality following ischaemic stroke” in Chapter 6) but rising obesity and diabetes threatens progress in tackling cerebrovascular disease (OECD, 2015).
Mortality rates are based on numbers of deaths registered in a country in a year divided by the size of the corresponding population. The rates have been directly age-standardised to the 2010 OECD population (available at http://oe.cd/mortality) to remove variations arising from differences in age structures across countries and over time. The source is the WHO Mortality Database.
Deaths from ischaemic heart disease are classified to ICD-10 codes I20-I25, and cerebrovascular disease to I60-I69.
References
Feigi, V. et al. (2016), “Global Burden of Stroke and Risk Factors in 188 Countries, During 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013”, The Lancet Neurology, Vol. 15, pp. 913–924.
OECD (2015), Cardiovascular Disease and Diabetes: Policies for Better Health and Quality of Care, OECD Publishing, Paris, https://doi.org/10.1787/9789264233010-en.
OECD (2012), OECD Reviews of Health Care Quality: Korea – Raising Standards, OECD Publishing, Paris, https://doi.org/10.1787/9789264173446-en.