Financing of health care
Health care can be paid for through a variety of financing arrangements. In some countries, health care might be predominantly covered by government schemes by which individuals are automatically entitled to care based on their residency. In other cases, compulsory health insurance schemes (either through public or private entities) finance the bulk of health spending. In addition to these, a varying proportion of health care spending consists of payments by households (either as standalone payments or as part of co-payment arrangements) as well as various forms of voluntary health insurance intended to replace, complement or supplement automatic or compulsory coverage.
In all but one OECD country, government schemes and compulsory health insurance constitute the main health care financing arrangements. Together they accounted, on average, for almost three-quarters of all health care spending across the OECD in 2015 (Figure 7.6). In Denmark, Sweden and the United Kingdom, central, regional or local government financed 80% or more of all health spending. In Germany, Japan, France and the Slovak Republic more than 75% of all health expenditure was paid for through compulsory health insurance. Only in the United States was less than half of all health spending financed by government or compulsory health insurance. By contrast, a large proportion of health spending (35%) was paid for via voluntary health insurance.
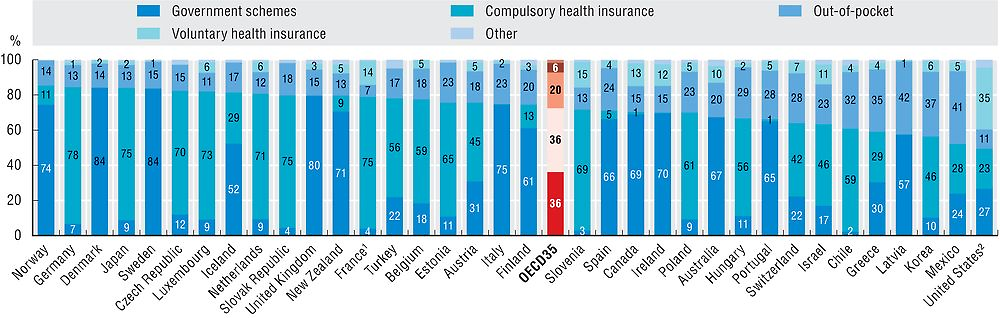
1. France does not include out-of-pocket payments for inpatient LTC thus resulting in an underestimation of the out-of-pocket share.
2. Spending by private health insurance companies in the United States is reported under voluntary health insurance.
Source: OECD Health Statistics 2017.
Governments provide a multitude of public services out of their overall budgets. Hence, health care is competing with many other sectors such as education, defence and housing. The size of public funds allocated to health is determined by a number of factors including, among others, the type of system in place and the demographic composition of the population. Relative budget priorities may also shift from year to year as a result of political decision-making and economic effects. In 2015, health spending by government schemes and compulsory insurance stood at around 15% of total government expenditure across the OECD (Figure 7.7). In Japan, Switzerland, New Zealand, the United States and Germany more than 20% of public spending was dedicated to health care. On the other hand, less than one out of every ten euros spent by governments or compulsory health insurance was allocated to health care in Latvia and Greece.
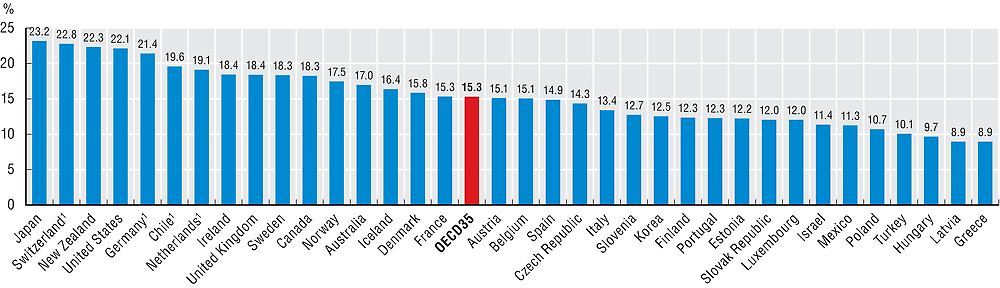
Note: Relating spending from government and compulsory insurance to total government expenditure may lead to an overestimation in countries where compulsory insurance is provided by private insurers.
1. Includes spending by private health insurers for compulsory insurance.
Source: OECD Health Statistics 2017, OECD National Accounts Database.
After government schemes and compulsory health insurance, the main source of funding tends to be out-of-pocket payments. On average across the OECD, private households directly financed around one-fifth of all health spending in 2015. This share is above a third of health spending in Greece (35%), Korea (37%), Mexico (41%) and Latvia (42%), while in France it is below 10%. With the implementation of universal health coverage in some OECD countries over previous decades, there have been some significant reductions in the share of health care costs payable by households. More recently, the share of out-of-pocket spending has been generally stable but with some notable increases in some European countries (Figure 7.8). In Greece (+6.2 percentage points) and Spain (+4.7 pp) the share of health spending payable by households has increased since 2009 due to the implementation of reforms to balance public budgets which shifted some financing responsibilities to patients. On the other hand, this share has been reduced in Mexico (-6.0 pp) and Chile (-2.3 pp) over the same time period.
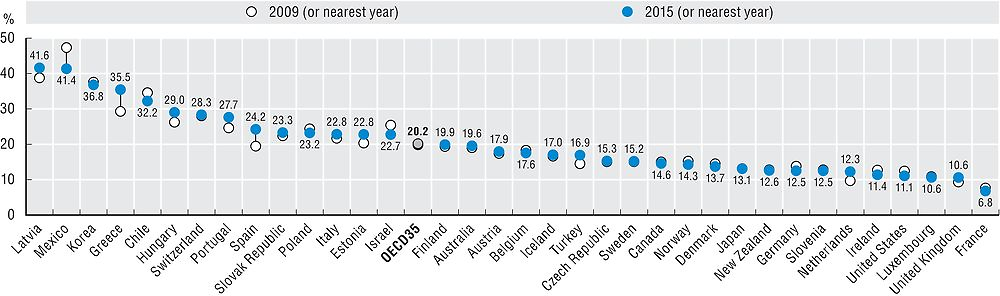
Source: OECD Health Statistics 2017.
Health care financing can be analysed from the point of view of financing schemes (financing arrangements through which health services are paid for and obtained by people, e.g. social health insurance), financing agents (organisations managing the financing schemes, e.g. social insurance agency), and types of revenues (e.g. social insurance contributions). Here “financing” is used in the sense of financing schemes as defined in the System of Health Accounts (OECD, Eurostat and WHO, 2011) and includes government schemes, compulsory health insurance as well as voluntary health insurance and private funds such as households’ out-of-pocket payments, NGOs and private corporations. Compulsory health insurance can be offered by private insurers, in some cases without an obligation to contract individuals (e.g. in Chile and Germany). Out-of-pocket payments are expenditures borne directly by patients and include cost-sharing arrangements and any informal payments to health care providers.
Total government expenditure is as defined in the System of National Accounts and includes intermediate consumption, compensation of employees, interest, social benefits, social transfers in kind, subsidies, other current expenditure and capital expenditure payable by central, regional and local governments as well as social security funds. Relating spending from government financing schemes and compulsory insurance schemes to total government expenditure is overestimated to a certain extent for those countries with compulsory health insurance provided by private insurers.
Spending by private health insurance companies in the United States are considered under voluntary health insurance although the Affordable Care Act (ACA) constitutes a mandate for individuals to buy health insurance or pay a penalty since 2014.
References
Mueller, M. and D. Morgan (2017), “New Insights into Health Financing: First Results of the International Data Collection Under the System of Health Accounts 2011 Framework”, Health Policy, Vol. 121, No. 7, pp. 764–769.
OECD/Eurostat/WHO (2017), A System of Health Accounts 2011: Revised edition, OECD Publishing, Paris, https://doi.org/10.1787/9789264270985-en.