Diabetes care
Diabetes is a chronic disease that occurs when the body’s ability to regulate excessive glucose levels in the blood is diminished. It is a leading cause of cardiovascular disease, blindness, kidney failure and lower limb amputation. Globally it is estimated that over 400 million adults had diabetes in 2015 and by 2040 it is projected this will grow to over 640 million adults. Diabetes caused 5 million deaths in 2015 (IDF, 2015).
Ongoing management of diabetes usually involves a considerable amount of self-care, and therefore, advice and education are central to the primary care of people with diabetes. Effective control of blood glucose levels through routine monitoring, dietary modification and regular exercise can reduce the onset of serious complications and the need for hospitalisation. Management of other key risk factors such as smoking, blood pressure and lipid levels are also important in reducing complications of diabetes.
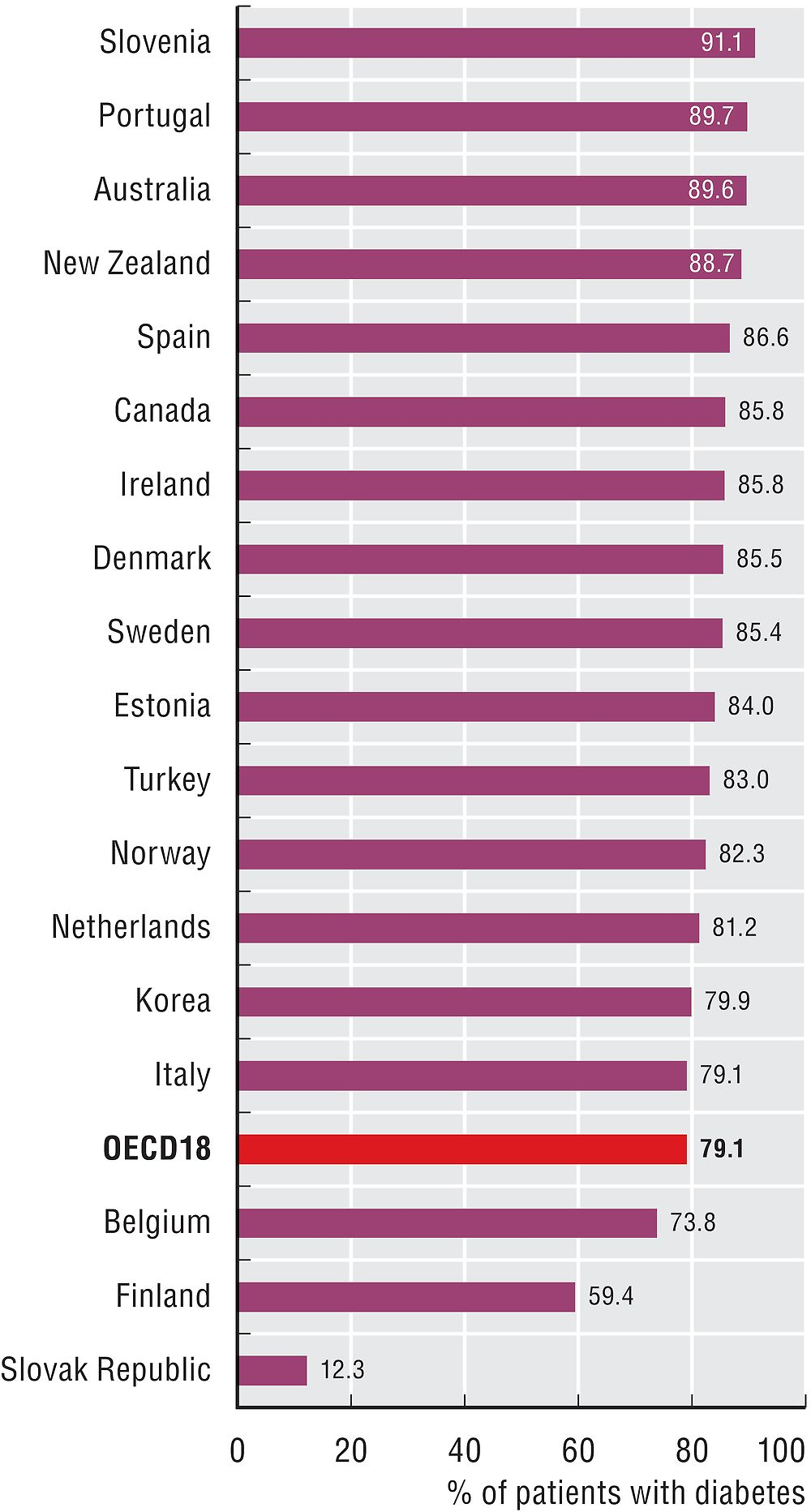
In diabetic individuals with hypertension, angiotensin-converting enzyme inhibitors (ACE-I) or angiotensin receptor blockers (ARB) are recommended in most national guidelines as first-line medications to reduce blood pressure. Figure 6.12 reveals there is broad consistency in the proportion of diabetic patients on recommended antihypertensive medications, with only Korea, Italy, Finland, Belgium and the Slovak Republic with rates less than 80%.
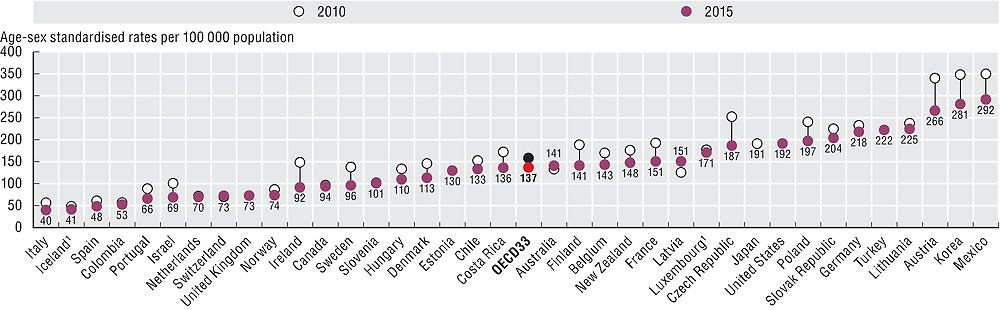
Figure 6.11 shows avoidable hospital admissions for diabetes. While admissions have fallen in many countries over time, more than a 7-fold variation in the rates is still evident across countries. Italy, Iceland and Spain report the lowest rates with Austria, Korea and Mexico reporting rates at least two times that of the OECD average. Prevalence of diabetes may explain some of the variation in rates. A positive relationship can be demonstrated between overall hospital admissions and admissions for diabetes, providing some indication that access to hospital care can also play a role in explaining international variation (OECD, 2015).
1. Three-year average.
Source: OECD Health Statistics 2017.
Note: Data for Canada only includes provinces of British Columbia, Manitoba and Saskatchewan.
Source: OECD Health Statistics 2017.
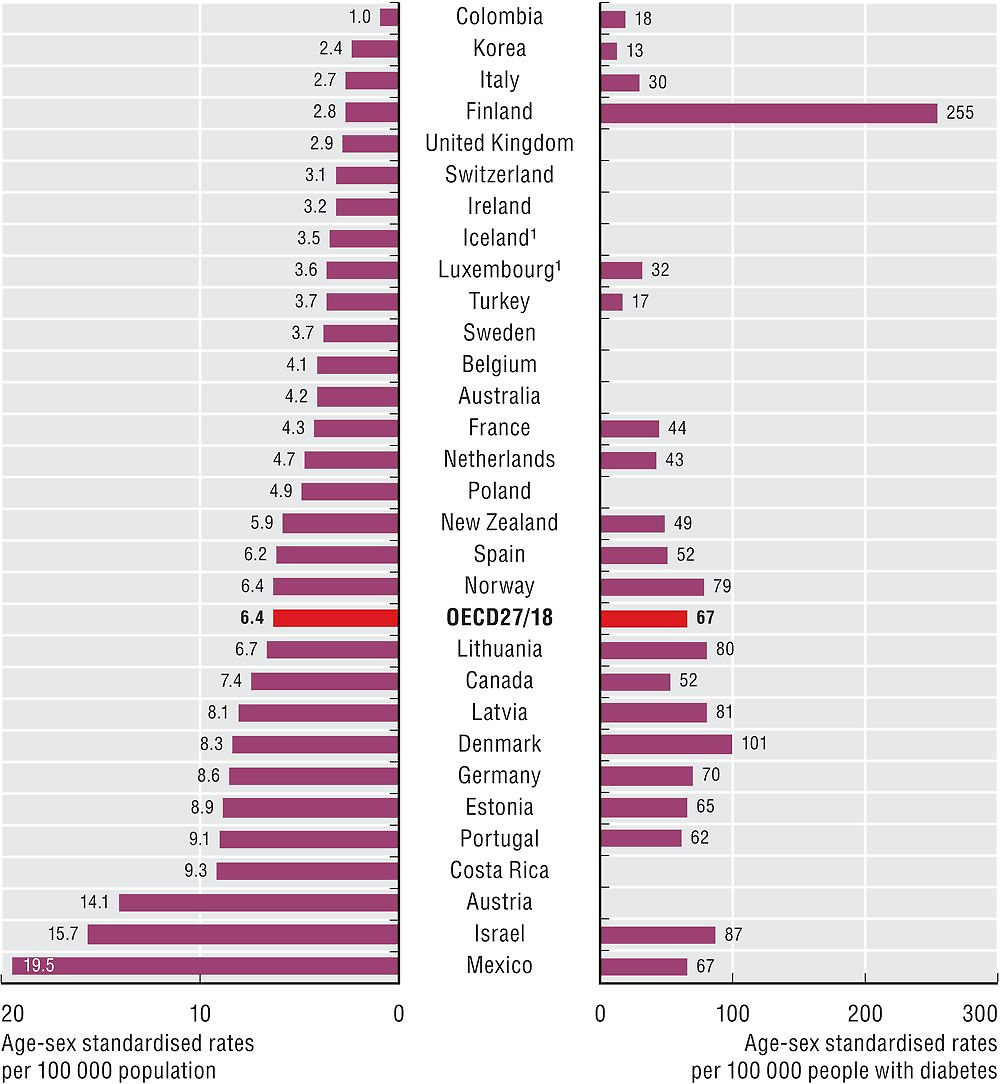
Hospital admissions for major lower extremity amputation reflect the long-term quality of diabetes care. Figure 6.13 shows the rates of amputation in adults with diabetes. In the left panel the rates based on the general population are presented. The international variation in rates is over 14-fold, with Colombia, Korea, Italy, Finland, and the United Kingdom reporting rates lower than 3 per 100 000 general population and Austria, Israel and Mexico reporting rates above 14. In the right panel rates based on the estimated diabetic population are presented. The rates based on the diabetic population are 9-fold higher than for the general population and display differences in the ranking of countries, providing an indication that differences in disease prevalence across countries may explain some, but not all, cross-country variation. In OECD countries, rates of amputation have declined significantly since 2000 (Carinci et al., 2016).
1. Three-year average.
Source: OECD Health Statistics 2017.
People with diabetes who have first choice antihypertensive medication prescriptions is defined as the number of people that have one or more prescriptions of an angiotensin converting enzyme inhibitor (ACE-I) or angiotensin receptor blocker (ARB) among people who are long term users of glucose regulating medication (people with diabetes) who also have one or more prescriptions per year from a range of medications often used in the management of hypertension.
Diabetes avoidable admission is based on the sum of three indicators: admissions for short-term and long-term complications and for uncontrolled diabetes without complications. The indicator is defined as the number of hospital admissions with a primary diagnosis of diabetes among people aged 15 years and over per 100 000 population. Major lower extremity amputation in adults with diabetes is defined as the number of discharges of people aged 15 years and over per 100 000 population, for the general population and the estimated population with diabetes. Rates for these indicators have been directly age-standardised to the 2010 OECD population.
Differences in data definition and coding practices between countries may affect the comparability of data. For example, coding of diabetes as a principal diagnosis versus a secondary diagnosis varies across countries. This is more pronounced for diabetes than other conditions, given that in many cases admission is for the secondary complications of diabetes rather than diabetes itself. Diabetes population estimates used to calculate the amputation indicators were self-reported by countries. Differences in data coverage of the national hospital sector across countries may also influence indicator rates.
References
Carinci, F. et al. (2016), “Lower Extremity Amputation Rates in People with Diabetes as an Indicator of Health Systems Performance. A Critical Appraisal of the Data Collection 2000–2011 by the Organization for Economic Cooperation and Development (OECD)”, Acta Diabetologica, Vol. 53, pp. 825-832.
IDF – International Diabetes Federation (2015), IDF Diabetes Atlas Seventh Edition 2015, www.diabetesatlas.org.
OECD (2015), Cardiovascular Disease and Diabetes: Policies for Better Health and Quality of Care, OECD Health Policy Studies, OECD Publishing, Paris, https://doi.org/10.1787/9789264233010-en.