Smoking
Tobacco kills nearly 6 million people each year, of whom more than 5 million are from direct tobacco use and more than 600 000 are non-smokers exposed to second-hand smoke. Tobacco is a major risk factor for at least two of the leading causes of premature mortality – cardiovascular diseases and cancer, increasing the risk of heart attack, stroke, lung cancer, cancers of the larynx and mouth, and pancreatic cancer, among others. In addition, it is a dominant contributing factor for respiratory diseases such as chronic obstructive pulmonary disease. Smoking in pregnancy can lead to low birth weight and illness among infants. Smoking remains the largest avoidable risk factor for health in OECD countries and worldwide.
Definition
The proportion of daily smokers is defined as the percentage of the population aged 15 years and over who report smoking every day.
Comparability
International comparability is limited due to the lack of standardisation in the measurement of smoking habits in health interview surveys across OECD countries. Variations remain in the age groups surveyed, the wording of questions, response categories and survey methodologies (e.g. in a number of countries, respondents are asked if they smoke regularly, rather than daily; and if they smoke cigarettes rather than all types of tobacco). In addition, self-reports of behaviours may suffer from social desirability bias that may potentially limit cross-country comparisons.
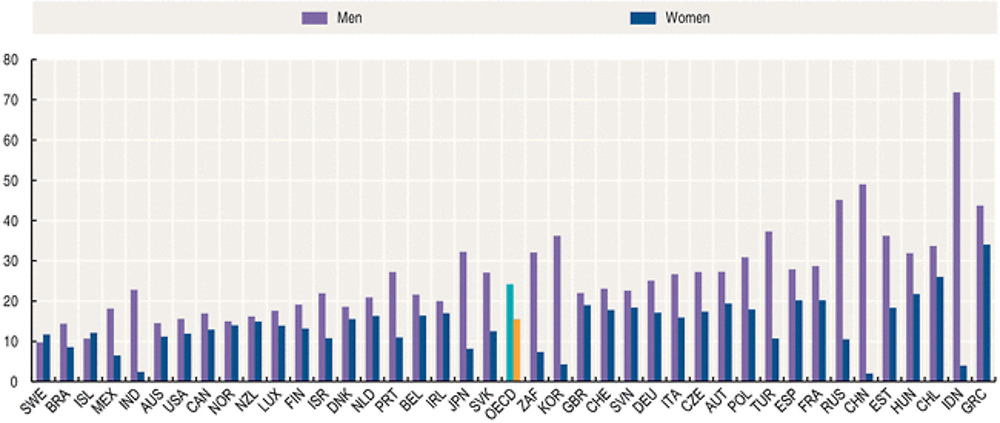
The proportion of daily smokers in the adult population varies greatly, even between neighbouring countries. Nineteen of 34 OECD countries had less than 20% of the adult population smoking daily in 2013. Rates were lowest in Sweden, Iceland, Mexico and Australia (less than 13%). Rates were also less than 13% in Brazil and India, although the proportion of smokers among men is high in India at 23%. On the other hand, smoking rates remain high in Greece in both men and women, and in Indonesia where more than one in two men smoke daily. Smoking prevalence is higher among men than among women in all OECD countries except in Sweden and Iceland. The gender gap in smoking rates is particularly large in Korea, Japan and Turkey, as well as in Russia, India, Indonesia, South Africa and China.
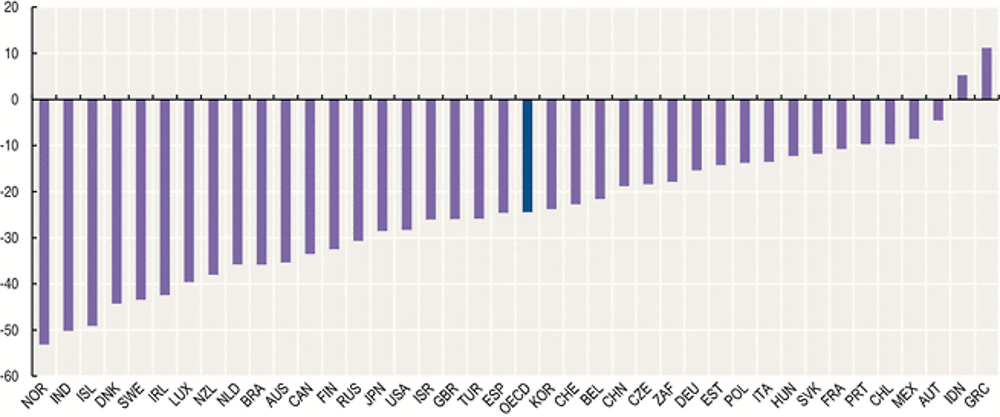
Since 2000, smoking rates across most OECD countries have continued to decline, although other forms of smokeless tobacco use, such as snuff in Sweden, are not taken into account. On average, smoking rates have decreased by about one fourth since 2000, from 26% to 20% in 2013. Large reductions occurred in Norway, Iceland, Denmark, Sweden and Ireland, as well as in India.
Much of the decline in tobacco use can be attributed to policies aimed at reducing tobacco consumption through public awareness campaigns, advertising bans, increased taxation, and restriction of smoking in public spaces and restaurants, in response to rising rates of tobacco-related diseases. As governments continue to reinforce their anti-tobacco policies, new strategies such as plain packaging for tobacco products aimed to restrict branding have been implemented (e.g. in Australia) and are being adopted by an increasing number of countries.
There is strong evidence of socio-economic differences in smoking and mortality. People in less affluent social groups have a greater prevalence and intensity of smoking and a higher all-cause mortality rate and lower rates of cancer survival.
Sources
-
OECD (2015), OECD Health Statistics (Database).
Further information
Analytical publications
-
OECD (2015), Cardiovascular Disease and Diabetes: Policies for Better Health and Quality of Care, OECD Publishing.
-
OECD (2013), Cancer Care: Assuring Quality to Improve Survival, OECD Publishing.
Statistical publications
-
OECD (2015), Health at a Glance, OECD Publishing.
-
OECD (2014), Health at a Glance: Asia/Pacific, OECD Publishing.
-
OECD (2014), Health at a Glance: Europe, OECD Publishing.
Websites
-
Health at a Glance (supplementary material), www.oecd.org/health/healthataglance.
-
Health Care Quality Indicators - Cardiovascular Disease and Diabetes, www.oecd.org/els/health-systems/hcqi-cardiovascular-disease-and-diabetes.htm.
-
OECD Health Statistics (supplementary material), www.oecd.org/els/health-systems/health-statistics.htm.