
Mortality following acute myocardial infarction (AMI)
Mortality due to coronary heart disease has declined substantially over recent decades (see indicator “Mortality from circulatory diseases” in Chapter 3). Reductions in smoking (see indicator “Smoking among adults” in Chapter 4) and improvements in treatment for heart diseases have contributed to these declines (OECD, 2015[23]). Despite this progress, AMI (heart attack) remains the leading cause of cardiovascular death in many OECD countries, highlighting the need for further reductions in risk factors and care quality improvements (OECD/The King's Fund, 2020[24]). The COVID-19 crisis has also revealed the need to maintain access to high-quality acute care for AMI during public health emergencies.
Metrics of 30-day mortality after AMI hospital admission are reflective of processes of care, such as timely transport of patients and effective medical interventions. However, the indicator is influenced not only by the quality of care provided in hospitals but also by differences in the patterns of hospital transfers, length of stay and AMI severity across countries.
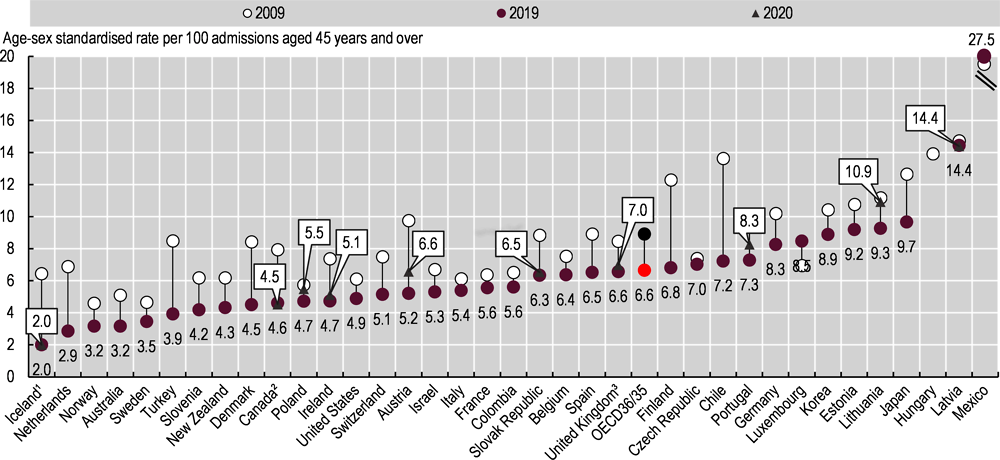
Figure 6.15 shows mortality rates within 30 days of admission to hospital for AMI using unlinked data – that is, only counting deaths that occurred in the hospital where the patient was initially admitted. The lowest rates in 2019 were in Iceland, the Netherlands, Norway, Australia, Sweden, and Turkey (less than 4% among patients aged 45 and over) while the highest rates were in Latvia and Mexico (over 13%). In Mexico, the absence of a co-ordinated system of care between primary care and hospitals may contribute to delays in reperfusion and low rates of angioplasty (Martínez-Sánchez et al., 2017[25]).
Figure 6.16 shows the same 30-day mortality rate but calculated based on linked data, whereby the deaths are recorded regardless of where they occurred after hospital admission (in the hospital where the patient was initially admitted, after transfer to another hospital or after being discharged). Based on these linked data, the AMI mortality rates in 2019 ranged from 3% in the Netherlands to 17% in Latvia.
Case fatality rates for AMI decreased substantially between 2009 and 2019, according to both datasets (Figure 6.15 and Figure 6.16). Across OECD countries, the average rate fell from 8.7% to 6.6% for same-hospital deaths and from 11.4% to 8.8% for deaths in and out of hospital. Between 2019 and 2020, however, case fatality rates increased in Lithuania, Poland and England (United Kingdom), while the rates were stable in countries including Canada, Iceland, Ireland, Latvia, Portugal and the Slovak Republic.
Changes in the trend reflect challenges faced by health systems in ensuring timely access to acute care during the COVID-19 crisis. In all countries reporting 2020 data, the number of people admitted to hospital due to AMI decreased. Reductions were particularly large in Canada and Portugal. Fewer AMI admissions and reductions in the number of procedures to treat heart attack were reported in Austria, Italy, Spain and the United States. These may be the result either of reduced hospital use from patients (due to concern about COVID-19 exposure or not wanting to burden the health system) or of ambulance systems not being able to transfer all patients promptly due to a surge in demand for COVID-19 patients. The absolute number of people who died of AMI within 30 days of hospital admission decreased substantially in Portugal, suggesting that at least some AMI patients may have died at home or in long-term care institutions before arriving at hospital.
Supplementary data are needed to assess the impact of COVID-19 on acute care for AMI and to support health systems in providing high-quality acute care during public health emergencies. England (United Kingdom) found that the number of ambulance callouts for heart attack was stable compared to previous years (Holmes et al., 2020[26]), and that while ambulance response times increased, this was not related to delays for revascularisation once in hospital and higher mortality (Little et al., 2020[27]). When resources are limited, more granular data such as hospital admissions and case fatality rates by AMI severity could further inform ways to promote effective provision and management of acute care – particularly for patients with the most severe conditions.
The case fatality rate measures the percentage of people aged 45 and over who die within 30 days following hospital admission for a specific acute condition. Unlinked data include only deaths that occurred in the same hospital as the initial admission; linked data include deaths recorded regardless of where they occurred, including in another hospital or outside the hospital where AMI was first recorded. The linked data-based method is considered more robust than the rates based on unlinked data, and results in much lower variations between countries. However, it requires a unique patient identifier to link the data across the relevant datasets, which is not available in all countries.
Rates are age- and sex-standardised to the 2010 OECD population aged 45 and over admitted to hospital for AMI, using International Classification of Diseases, tenth revision (ICD-10) codes I21-I22.
1. Three-year average for all years except 2020. 2. 2020 estimate based on provisional 1 April to 30 September data from all jurisdictions except Quebec. 3. 2020 data are provisional and include England only.
Source: OECD Health Statistics 2021.

1. Three-year average for all years except 2020. 2. Data do not include deaths outside acute care hospitals. 2020 estimate based on provisional 1 April to 30 September data from all jurisdictions except Quebec. 3. 2020 data are provisional and include England only.
Source: OECD Health Statistics 2021.