4. The Irish paradox: Doctor shortages despite high numbers of domestic and foreign medical graduates
Ireland has the highest number of medical graduates per population among OECD countries, but half of the students come from other countries. The number of international students is not subject to the numerus clausus policy that limits the entry of Irish students into medical education, and the medical schools have become increasingly dependent on the tuition fees international students pay. However, the large student numbers are not matched by opportunities to complete an internship and postgraduate training. To the contrary, the number of internship places for international medical students has fallen as national authorities reserve a greater proportion for the growing number of Irish medical graduates to ensure a good return on the public investment in their education. Thus, most international students try to complete their medical education and enter postgraduate training outside Ireland. Also, many Irish medical graduates and (newly trained) doctors seek training and job opportunities abroad. Hence, while Ireland provides initial medical education to a large number of students, since many leave the country after graduation, it nonetheless relies heavily on international recruitment of doctors to fill its domestic needs. More coherent education, training, and employment policies are needed to address this paradox.
4.1. Introduction
Ireland has a long-standing tradition of hosting international medical students. In 2017/18, international students – most coming from outside the European Union/European Free Trade Association (EU/EFTA) – accounted for half the medical student body. This contributes to Ireland producing the highest number of medical graduates per population among all EU and OECD countries.
Irish medical schools are able to attract and admit a large number of international students because of their good reputation and also because these students are not subject to the numerus clausus policy that limits the entry of Irish and other EU/EFTA students into medical education. Medical schools in Ireland have become increasingly dependent on the additional income from the high tuition fees that non-EU/EFTA students pay.
However, the expansion in medical student numbers has not been matched by an expansion in the number of internship opportunities the students need to complete their education and obtain the right to practice as a doctor in Ireland. To the contrary, the number of internship places for international medical students has diminished greatly as national authorities have reserved a greater proportion for the growing number of Irish and other EU/EFTA medical graduates. This means that most international graduates of Irish medical schools need to leave the country if they are to earn the right to practice. Furthermore, many Irish medical graduates and doctors also emigrate in search of training and work opportunities abroad.
As a result, Ireland faces a paradoxical situation whereby it educates a large number of domestic and international medical students, but since many leave the country after graduation, it has to rely heavily on international recruitment of fully-trained doctors to meet its domestic demand. Indeed, the proportion of foreign-trained doctors in Ireland rose substantially to 42% in 2016 – the second highest among the OECD countries.
Against this background, this chapter describes findings from a case study on the internationalisation of medical education in Ireland – in particular its dynamics, magnitude, and main drivers as well as the views on the current situation of the main stakeholders in the medical education and health sectors. The discussion in this document relates to international medical students enrolled in long-cycle programmes. The study was undertaken in 2018 and is based on key-informant interviews with representatives of the main policy actors in the education and health sectors in Ireland – including government departments, regulatory bodies, professional associations, and medical schools (see Annex Table 4.A.2 for a complete list of interviewees’ institutional affiliations) – in addition to a literature review. The perspectives of a sample of non-EU/EFTA graduates of Irish medical schools were also captured through an online survey and by email. Moreover, researchers from the Health Workforce Research Group (Royal College of Surgeons in Ireland) and the Doctor Retention and Motivation Project (Royal College of Physicians of Ireland) provided additional information and perspective.
4.2. International students account for half of all medical students in Ireland
In 2016, Ireland had the highest number of medical graduates per population of all OECD and EU countries, 24.4 per 100 000 population. This is approximately twice the figure in the United Kingdom (12.9) and the OECD average (12.5). Ireland has, at least for the past decade, produced relatively more medical graduates than nearly all other OECD countries (Figure 4.1).
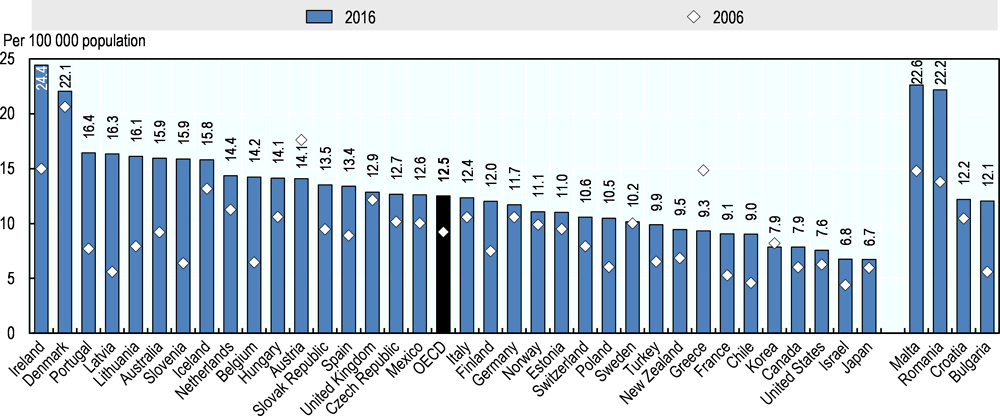
Notes: In Denmark, Mexico, New Zealand, and Sweden, the data refer to new doctors receiving an authorisation to practise, which may result in an overestimation if these include foreign-trained doctors. The countries on the right-hand side of the figure are EU countries that are not OECD members. There were no medical graduates in Luxembourg in 2016.
Source: OECD Health Statistics 2018, https://doi.org/10.1787/health-data-en.
About half of the medical student body in Ireland, however, consists of international students. All six Irish medical schools have large numbers of international students. The Royal College of Surgeons in Ireland has the largest number and share of international students; they accounted for more than three-quarters (78%) of all students in the academic year 2017/18 (Table 4.1).
This proportion of international medical students is much higher than the average in all tertiary education programmes in Ireland, where international students account for 8% of total enrolments and 15% of enrolments in master’s (or equivalent) programmes (OECD, 2018[1]).
4.2.1. Canadians are the most numerous group of international medical students in Ireland
In 2017/18, Canadians were the most numerous international medical students (29% or 993 of the total number of international enrolments), followed by students from Malaysia (19% or 667 enrolments) (Table 4.2). According to statistics of the Higher Education Authority (Health Education Authority, 2018b[3]), the total number of Canadian students enrolled in Irish medical schools nearly tripled in the past decade, from 381 in 2006/07 to 993 in 2017/18.1
4.3. Admission rules and tuition fees differ for Irish and EU/EFTA students and those from non-EU/EFTA countries
4.3.1. Non-EU/EFTA students face no numerus clausus policy for entry into medical education but have limited access to internships
In Ireland, the medical education begins with a medical degree programme of between four and six years, followed by a 12-month internship (Figure 4.2). Students entering their medical education directly from secondary school complete a course of between five and six years,2 while graduate-entry programmes – offered since 2006 – are four years in duration. The graduate medicine programmes are open to students who have already completed a degree (bachelor’s or higher) in another discipline.
In addition to the medical degree, graduates must complete a 12-month internship to obtain the right to practise medicine in Ireland. The National Doctors Training and Planning unit (NDTP) within the Health Service Executive (HSE) has the responsibility for the intern-matching scheme (see Annex Table 4.A.1 for a description of governance and responsibilities of the various actors in medical education and training in Ireland). The internships are delivered in clinical sites organised in six intern-training networks, each based around one of the medical schools. During the internship, graduates are employed and paid by the HSE. On successful completion, the graduate may proceed to postgraduate specialist training (NDTP, 2017[4]; Health Service Executive, 2018[5]).
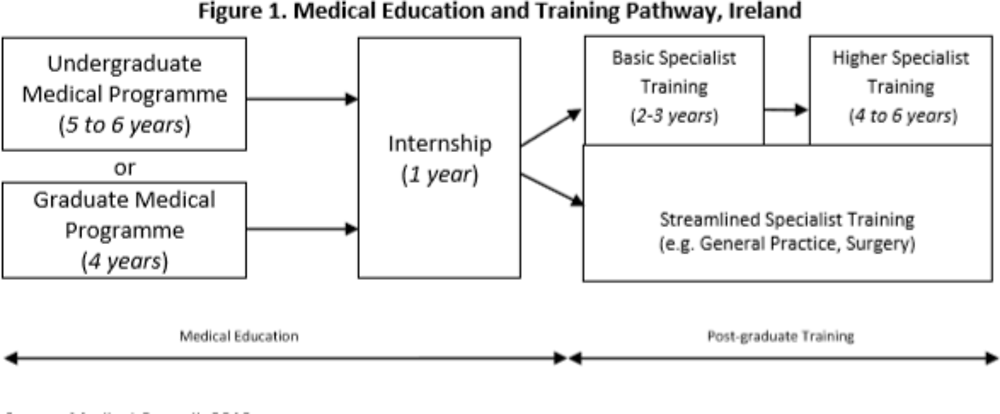
Source: Medical Council, 2013[6].
Like most other OECD countries, Ireland has two numerus clausus systems regulating the number of places for the initial medical education and for the subsequent internship, respectively. The first, related to the entry of students into medical education programmes, applies only to Irish students and other nationals of EU/EFTA countries but not to students from non-EU/EFTA countries.3
Between 2006 and 2016, the intake of students subject to the numerus clausus policy increased steadily, leading to a more than two-fold increase in the number of Irish (and other EU/EFTA) medical graduates – from 370 in 2006 to 854 in 2016 (of which 7% (61) were from other EU/EFTA countries) (Health Education Authority, 2018b[7]). This increase followed the recommendation of a 2006 government report that called for an expansion to reduce the reliance on foreign-trained doctors.
At the same time, the number of non-EU/EFTA medical graduates increased even more rapidly – more than three-fold: from 140 in 2006 to 479 in 2016 – in line with the strategies of Irish medical schools to recruit more students from abroad (Health Education Authority, 2018b[7]). However, the current intern-matching procedure (in place since 2015) prioritises Irish and other EU/EFTA nationals in the first round. This arrangement has been adopted to protect the public investment in the education of these students (Box 4.1) (NDTP, 2017[4]).
Between 1978 and 2006, the intake of Irish and other EU/EFTA medical students was capped at 305 per year. During this time, the gap between the supply of and demand for doctors was closed by recruiting from overseas (Campbell, 2015[8]). A 2006 government report, known as the Fottrell Report, recommended that the intake of Irish and EU/EFTA students should be increased to approximately 725 students per year, based on an assessment of the medical workforce required to move towards national self-sufficiency (Department of Health, 2006[9]).
The Fottrell Report also noted that the high number of non-EU/EFTA students in Irish medical schools was unusual among developed countries and saw this as potentially limiting the clinical training placements available to the growing numbers of Irish and other EU/EFTA medical students. It therefore recommended that “the proportion of non-EU students entering clinical training should be no greater than 25% of total student intake”. The report also stated that the intake strategy “appears to be based on attracting high numbers of non-EU students into medical school because the income generated is essential to maintain the viability of the schools and to subsidise the education of EU and Irish students.” This strategy of accepting a high number of international students is ongoing, however.
In 2006, 488 internship places were available, of which 31% were occupied by non-EU/EFTA graduates of Irish medical schools. The report noted that these graduates “in most cases are not likely to remain with the Irish Health Service following internship and full registration”.
The number of internship places increased from 488 in 2006 to 727 in 2015 (as recommended in the report), but fears remained that increasing numbers of applicants from non-EU/EFTA countries would result in insufficient places for Irish and other EU/EFTA graduates. A decision was therefore made in 2015, following an engagement between the NDTP and the Department of Health, to prioritise Irish and other EU/EFTA graduates from Irish medical schools in the first round of the intern-matching process to protect the public investment in education of those students (NDTP, 2017[4]), thereby reducing greatly the opportunities for non-EU/EFTA graduates to get a place.
Source: (Department of Health, 2006[9]).
Accordingly, in 2016 there were 1 191 applicants for the 727 available internship places, of which:
-
93% (678) were allocated to graduates of Irish medical schools with Irish (or other EU/EFTA country) citizenship;
-
5% (34) were allocated to other EU/EFTA nationals who had completed their medical studies in other EU/EFTA countries (including Irish nationals who had completed their medical degrees abroad);
-
only 2% (15) were allocated to non-EU/EFTA graduates, including those who had completed their first medical degree in Ireland (NDTP, 2017[4]).
In consequence, the majority of non-EU/EFTA graduates of Irish medical schools cannot complete their education and, thus, cannot obtain a full registration to practise as a doctor in Ireland; they are also thereby automatically barred from any access to postgraduate specialist training. These graduates likely seek the internship and specialist training in their home or third countries, but their success rate is not documented. Such a situation bears a risk of “brain waste”, if these international medical graduates are not able to complete their training and practice as a doctor.
4.3.2. The selection process for non-EU/EFTA candidates is separate
Irish and other EU/EFTA students are admitted to medical schools through the Central Applications Office. Each medical school sets a minimum subject and points requirement in the Irish leaving certificate or equivalent exam. Candidates must also successfully pass the health professions admission test for Ireland (HPAT-Ireland). The allocation of places for medicine is determined based on a combination of the leaving certificate (or equivalent) and the HPAT-Ireland score (Central Applications Office, 2018a[10]). Graduate-entry students must fulfil a minimum academic requirement in terms of the degree they have obtained and must sit the graduate medical schools admissions test (Central Applications Office, 2018b[11]).
The admission of non-EU/EFTA students is based on a separate competitive selection process, which varies according to the university and/or the region from which the application is made. In general, universities set minimum academic eligibility criteria, including an English language requirement. For graduate-entry programmes, a minimum requirement is a bachelor’s degree in addition to a minimum score from the graduate medical schools admissions test or medical college admissions test. Applications by non-EU/EFTA students are facilitated by dedicated agencies, established by the medical schools (Box 4.2).
Dedicated agencies, such as the Atlantic Bridge programme and the Irish Universities and Medical Schools Consortium, have been established to facilitate the application to Irish medical schools for non-EU/EFTA students.
Atlantic Bridge is the main partner for prospective students from North America (although students from other non-EU/EFTA countries can also apply through the programme). Students can apply to multiple medical schools via one application. All six Irish medical schools are part of the programme (Atlantic Bridge, 2018[12]).
The Irish Universities and Medical Schools Consortium facilitates the application for and the allocation of places for students from Malaysia and Singapore. Four of the six medical schools make up the Consortium (IUMC, 2018[13]), which began to focus on Malaysia and Singapore approximately 25 years ago, when it joined an Irish government trade delegation to Southeast Asia (UCD, 2018[14]).
4.3.3. Non-EU/EFTA students pay significantly higher tuition fees
Under the Free Fees Initiative, Irish and other EU/EFTA students do not pay tuition fees for full-time undergraduate courses in Ireland (Health Education Authority, 2018b[3]). However, universities charge a student contribution (a registration fee) of 3 000 euros (EUR) annually (Student Universal Support Ireland, 2018[15]). Moreover, an additional annual student levy is applied by some universities; for example, EUR 224 by the National University of Ireland, Galway (NUIG, 2018[16]) and EUR 475 by the Royal College of Surgeons in Ireland (RCSI, 2018[17]).
Graduate-entry students are not eligible for the Free Fees Initiative. This means that Irish and other EU/EFTA nationals who take the graduate-entry path into medicine typically pay annual tuition fees of approximately EUR 14 000 (Haugh, Doyle and O’Flynn, 2014[18]).
Medical students from non-EU/EFTA countries also pay tuition fees, which differ depending on the university and whether the student takes the undergraduate or graduate-entry path. Annual tuition fees paid by non-EU/EFTA students are between EUR 43 000 and EUR 56 500 (Table 4.3).
Under the Student Support Act 2011 (Government of Ireland, 2011[19]), some students are eligible for a government grant, depending on their nationality and financial means. Being eligible for a full grant means that either the annual student contribution charge or the tuition fee is covered in addition to a maintenance grant to cover living expenses up to a maximum of EUR 5 915 per year (Student Universal Support Ireland, 2018[15]). Graduate-entry students are not eligible for government grants.
Most international students fund their studies directly or through government loans from their home country or private loans:
-
American students are eligible for federal loans up to the cost of attendance (registration and tuition fees) each year, while
-
Canadian students can use a student line of credit for professional students or the Canada Student Loan Program (Atlantic Bridge, 2018a).
-
According to information from medical schools, some students from Malaysia and Singapore are also funded through (usually private) loans, but many cover their tuition fees out-of-pocket.
-
Only a small number of international students receive scholarships, which do not have to be repaid and which in nearly all cases are from their home country.
4.4. Medical schools in Ireland seized the opportunity to respond to the unmet demand from international students to study medicine
4.4.1. Push and pull factors for international students include restrictions on access in home countries and the reputation of Irish medical schools
International medical students and other stakeholders identified two main push factors in students’ home countries: a limited medical education capacity in some countries – in particular in Southeast Asia (despite the increase in the number of medical schools in Malaysia in the recent decades) – and numerus clausus policies limiting the intake into medical schools in other countries, such as Canada.
Without exception, the people interviewed for this study felt that the medical education and training in Ireland was of a high standard and that the reputation for the quality of education was a major attraction for students from overseas. There was also a general confidence that degrees from Irish medical schools would be widely recognised and would enable the entry into internships and residency programmes in foreign students’ home countries or in third countries around the world. In addition, the fact that the courses are given in English helps in attracting students from other English-speaking countries. At the same time, Irish medical schools have put much greater effort into marketing abroad in the last decade to attract more students (see Box 4.2).
Another important pull factor is the international student cohort itself, which offers unique networking opportunities. The multicultural student body is considered beneficial for growing accustomed to being a doctor in increasingly mixed patient communities and within a multicultural health workforce.
4.4.2. International students are an important source of income for medical schools
Some stakeholders – in particular medical school representatives – pointed to the underfunding of university education as a driver for increasing the number of international medical students (see also Box 4.1). Medical schools indicated that they have become increasingly dependent on the income derived from fees paid by international students, as public funding for domestic students has decreased over the past ten years. They mention, for example, that their world-renowned educational facilities have been financed partly from this additional income – among them the clinical simulation facility of the Royal College of Surgeons in Ireland.
The medical schools receive state funding through the HEA in the form of a block grant that covers fixed costs; they also receive grants for each Irish and other EU/EFTA student (Indecon, 2005[20]).4 A recent report of the Irish Universities Association highlighted, however, that the average state funding per student (Irish or other EU/EFTA) in universities and colleges in Ireland had fallen by 50% since 2008 (Irish Universities Association, 2018[21]).
According to estimates (Campbell, 2015[8]), each medical graduate costs an Irish medical school between EUR 105 000 and EUR 126 000, depending on the duration of their studies. This is reflected in and consistent with the medical schools’ opinion that the cost of teaching a medical student is approximately EUR 20 000 to EUR 25 000 a year. The schools stress that, since only approximately EUR 16 000 is covered by government grants, non-EU/EFTA students subsidise the education costs of Irish and other EU/EFTA students. As noted above, tuition fees for non-EU/EFTA students are between EUR 43 000 and EUR 55 600 per year.
The internationalisation of medical studies is also driven by the medical schools’ ambition to maintain their leading position in the global education market through close links with other countries (Box 4.3).
The medical schools’ international strategy includes the establishment of medical campuses or programmes abroad. The Royal College of Surgeons in Ireland (RCSI) and the University College Dublin, for example, partnered to establish the Penang Medical College in Malaysia in 1995. Under this programme, students spend the first half of their training (two years) in Dublin and the remainder in Penang. Approximately 310 students from Penang Medical College were in Ireland in 2018 (spread between RCSI and University College Dublin). Since 2011, RCSI has also delivered an undergraduate medicine programme in another medical school in Malaysia – the Perdana University. Moreover, in 2005 RCSI established a medical university in Bahrain, which delivers undergraduate programmes in medicine and undergraduate and master’s programmes in nursing (RCSI, 2018b[22]).
Medical schools are also involved in international initiatives at the postgraduate level, with the International Medical Graduate Training Initiative the largest effort, contributing to clinical training of 200 overseas doctors in 2016. The Initiative was established in 2013 as a collaboration between the HSE, the Royal College of Physicians of Ireland, and the College of Physicians and Surgeons of Pakistan (Brugha, Cronin and Clarke, 2018[23]). It enables overseas trainees to gain access to clinical training they cannot get in their home country, with the aim of enhancing the individual doctor’s clinical skills and, in the longer term, enhancing their domestic health services (trainees must return home after their training period of approximately two years to receive certification).
Training is now available in the specialties of anaesthesia, emergency medicine, general medicine, obstetrics/gynaecology, ophthalmology, paediatrics, psychiatry, and surgery (NDTP, 2018[24]). Since the Initiative began in 2013 with 28 trainees from Pakistan, it has expanded to take in trainees from Sudan and externally sponsored (by their country of origin) trainees from Kuwait, Saudi Arabia, Oman, and the United Arab Emirates (Walsh and Brugha, 2017[25]). Stakeholders saw this initiative as having clear benefits for all parties involved. Unfilled non-consultant hospital doctor posts in Ireland were converted to training posts, meeting a service need while offering international experience to the participating physicians in training.
4.5. Despite having the highest number of medical graduates relative to its population, Ireland is heavily reliant on foreign-trained doctors
Despite having the highest percentage of medical graduates in the population across all OECD countries (see Figure 4.1), Ireland employs a greater proportion of foreign-trained doctors than any other EU country: 42% of all doctors employed in Ireland in 2016 obtained at least their first medical degree in another country. Among all OECD countries, only Israel – a country of recent and ongoing immigration – has a greater proportion of foreign-trained doctors (58% in 2016). Furthermore, Ireland also ranks only 27th among the 36 OECD countries with regard to the number of doctors per capita, at 2.9 per 1 000 inhabitants in 2016 (see Figure 1.1 in Chapter 1).
This section describes trends in the number of foreign-trained doctors and provides some explanations for this paradoxical situation in Ireland, which delivers medical education to a large number of students but does not seem able to retain many of the international medical graduates or Irish doctors once they complete their clinical training.
4.5.1. The reliance on foreign-trained doctors in Ireland has increased
Because of both the lack of opportunity for international graduates of Irish medical schools to complete their education and postgraduate training in Ireland and the emigration of many newly trained Irish doctors, the country is increasingly reliant on foreign-trained medical practitioners to meet its needs. The proportion of foreign-trained doctors has risen substantially from 13% of all registered doctors in 2000 to 33% in 2010 and to 42% in 2016 – the second highest share among the OECD countries (see Table 1.3 in Chapter 1).
In 2017, among 9 606 foreign-trained doctors in Ireland (see also Figure 4.3):
-
2 057 (21%) trained in Pakistan – a more than 50% increase since 2011 (1 313);
-
1 228 (13%) trained in Sudan – more than twice as many as in 2011 (546);
-
758 (8%) trained in the United Kingdom – around 10% more than in 2011 (691);
-
733 (8%) trained in Romania – a more than three-fold increase since 2011 (226).
Moreover, a phenomenon observed in relation to the doctors trained in central European medical schools is that many are not nationals of their countries of training. For example:
-
more than one-fifth of the 164 Indian junior doctors working in non-consultant hospital doctor (NCHD) posts5 in Ireland in 2015 graduated from a medical school in Poland (see also Chapter 5);
-
over one-third (119 of 301) of doctors working in HSE posts (all posts in the public health service, including those occupied by medical trainees) in Ireland in 2015 who got their first degrees in Romania were nationals from outside the EU/EFTA/OECD – primarily from Pakistan, India, and Nigeria (Brugha, Cronin and Clarke, 2018[23]) (see also Chapter 6).
However, it is also of note that some Irish nationals who did not manage to get a place in a medical school in Ireland and therefore graduated abroad subsequently practise in Ireland. For example, of the 40 graduates of Czech medical schools working as doctors in Ireland in 2015, 13 were Irish nationals. This pattern has also been reported in the United Kingdom with respect to UK nationals (Brugha, Cronin and Clarke, 2018[23]).
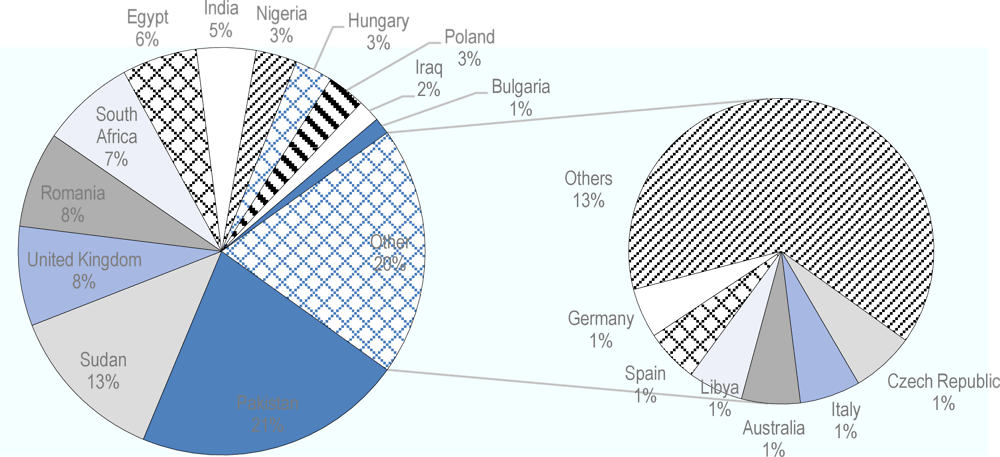
Note: Some data may be missing since not all countries of origin (training) are able to provide this migration data.
Source: OECD Health Statistics 2019, https://doi.org/10.1787/health-data-en.
4.5.2. High numbers of international and Irish medical graduates and fully-trained doctors emigrate
The vast majority of international graduates cannot proceed beyond their first medical degree and obtain the right to practise medicine in Ireland
As noted in Section 4.3.1, in addition to the medical degree, graduates must complete a 12-month internship to obtain the right to practise medicine in Ireland. However, the rules of the current intern-matching procedure mean that in practice the priority is given to Irish6 and other EU/EFTA nationals graduating from Irish medical schools in the first round of the process. Hence, only a few remaining internship places (2% out of 727 in 2016) are offered to students from non-EU/EFTA countries (NDTP, 2017[4]). As a result, nearly all international graduates of Irish medical schools move either back to their home country or to a third country, in the hope of completing their medical education. As also noted earlier, their success rate is not known as the career paths of these international graduates are not documented. Such a situation bears a risk of “brain waste”, if these international medical graduates are not able to complete their training and practice as a doctor.
Also many Irish medical graduates and doctors move to other countries
The interviewed stakeholders highlighted a long tradition of temporary emigration among Irish medical graduates and junior doctors, particularly to the United Kingdom and the United States. The pattern in the past was that many returned to Ireland to take up consultant posts once they had enhanced their skills and experience abroad.
In the last decade, however, the general perception is that the scale of emigration has increased and its character has changed from temporary to long-term (Humphries et al., 2017[27]). An analysis of Medical Council register data shows that, between 2012 and 2015, 6-9% of doctors aged 25-44 left the register annually (these numbers may include onward-migrating foreign-trained doctors – see also next sub-section). Most of these exits are believed to be doctors emigrating (Brugha, Cronin and Clarke, 2018[23]). Other data show that between 2008 and 2014 approximately 3 798 doctors previously registered in Ireland registered to practise and/or completed registration processes in five major destination countries (Australia, Canada, New Zealand, the United Kingdom, and the United States). This number exceeds the total number of Irish (or other EU/EFTA) graduates from Irish medical schools during the same period (Humphries et al., 2017[27]). More detailed data on Irish medical trainees reveal high rates of doctors working or training abroad within two years of their internship, or two years after they reported being in higher specialist training (Brugha, Cronin and Clarke, 2018[23]).
Moreover, approximately 400 of 3 140 (13%) permanent consultant posts were either vacant or filled on a temporary or agency basis in 2018 (Public Service Pay Commission, 2018[28]).7 Other research highlights the fact that vacant posts are also an issue in general practice, despite many general practitioners (GPs) remaining in post after retirement age (Brugha, Cronin and Clarke, 2018[23]).
Poor training experience and working conditions in general are the primary factors pushing Irish medical graduates, trainees, and doctors to migrate to other countries (Brugha, Cronin and Clarke, 2018[23]). Interviews also indicated the limited number of specialist training posts as another driver of outward migration. Although the number of Irish (and other EU/EFTA) graduates from Irish medical schools doubled between 2006 and 2015, the same period saw only a modest increase in the number of doctors enrolled in specialist training programmes (Brugha, Cronin and Clarke, 2018[23]): 2017 saw 704 enrolments in basic and streamlined specialist training programmes (NDTP, 2018b[29]).
Much has been written about the impact of issues related to training experience on the retention of Irish medical graduates and trainees: the associations between these poor experiences and the intention to leave and not return are strong and significant (Brugha, Cronin and Clarke, 2018[23]). In this context, there has been some progress on related recommendations issued by the Department of Health (2014) – for example, in streamlining the training and increasing the flexibility in training opportunities (NDTP, 2018b[29]). Challenges persist, however, including a lack of designated training time, performance of non-core tasks (below the trainees’ skill level), and an inconsistency in intern induction practices. Moreover, the shortage of consultants and the inconsistent structuring of their participation in training have a negative impact on the quality (Brugha, Cronin and Clarke, 2018[23]).
Among the aspects of work that affect the retention of fully trained doctors negatively were mentioned high numbers of patients on waiting lists, understaffing, and complex work situations. Doctor wellbeing was also highlighted as a concern. Furthermore, stakeholders named a lack of work-life balance and high levels of stress, and referred to recent findings that 30% of doctors in Ireland are suffering from burnout (RCPI, 2017[30]).
A recent report on public service pay (Public Service Pay Commission, 2018[28]) confirms the difficulties in retaining Irish doctors and filling consultant posts, but concludes that remuneration is not the main issue. Nevertheless, the report points out that the consultants’ pay was reduced in 2012. The interviewed stakeholders estimated that consultants appointed after 2012 receive approximately 30% less pay than those appointed before 2012.
Many junior doctors with a foreign medical degree are employed in non-training posts and reemigrate in search of specialist training opportunities
In contrast to the high degree of internationalisation in undergraduate medical education, the number of international graduates in postgraduate specialist training schemes is relatively small. This is partly related to the difficulty in accessing internship positions for many international graduates of Irish medical schools (see Section 4.3.1).
It also reflects the fact that many foreign-trained junior doctors (medical graduates who have not yet completed specialist training) arriving in Ireland are employed in long-term non-training posts, such as NCHD posts in small hospitals that are not suitable for delivering specialist training. Indeed, foreign-trained doctors fill most of the NCHD non-training posts, as few Irish doctors apply for them.
In 2015, only 20% of those on the specialist trainee register had qualified outside Ireland; of the total number of NCHDs who were not in training nearly 80% (2 325) were graduates of a medical school outside Ireland (Medical Council, 2016) (Medical Council Annual report 2017, 2018[31]). In addition, there has been a greater increase in the number of NCHDs in non-training than in training posts (Public Service Pay Commission, 2018). There was a 15.8% increase in the total number of NCHDs (from 4 936 to 5 717) between 2011 and 2015, but a much larger (32%) rise in non-trainee NCHDs over the same period (Walsh and Brugha, 2017[25]). In 2015, the distribution of junior doctors between the training and non-training NCHD posts by nationality and country of training was a follows (Table 4.4):
-
Irish nationals represented less than half (49%) of the NCHDs working in Ireland in 2015.
-
Of these, 78% were registered in the specialist trainee scheme – i.e. they were on track to become a hospital consultant specialist or a GP.
-
Nationals of India, Nigeria, Pakistan, and Sudan accounted for over one-quarter (28%) of the NCHD workforce.
-
Most of these – 86% of the Sudanese, 80% of the Pakistani, 73% of the Indian, and 63% of the Nigerian NCHDs – were in non-training posts.
-
Regarding the place of training, nine out of ten Pakistani and Sudanese NCHDs trained in their own country, compared with around half of the Indian and Nigerian NCHDs (the other half trained predominantly in medical schools in central and eastern Europe) (see also Table 4.3).
-
One-third of the Malaysian NCHDs are in specialist trainee posts. This is an unusual group, as most (130 out of 156) graduated in Ireland.
Foreign-trained doctors report taking up service posts in Irish hospitals in the hope of career progression or accessing postgraduate training, but when this hope remains unrealised, and because of a fear of deskilling, the majority actively seek to migrate onwards or return home. A 2013 survey found, for instance, that almost half (47%) of all foreign-trained doctors in Ireland planned to reemigrate (Humphries et al., 2017[27]). Indeed, in 2015, the exit rate for foreign-trained doctors was 2-3 times higher than for graduates of Irish medical schools. On the other hand, many non-EU/EFTA nationals (especially from low- and middle-income countries) remain in non-training posts in smaller hospitals for years and sometimes decades (Brugha, Cronin and Clarke, 2018[23]).
As an exception, the specialist training opportunities for foreign-trained doctors are better in the GP training scheme than for other specialties. The interviewed stakeholders mentioned the requirement to exhaust the pool of EU/EFTA candidates before offers can be made to non-EU/EFTA applicants, but if a non-EU/EFTA candidate was not restrictive about the location of the training posts applied to, they had a good chance of being successful in their application. The trainee intake in this specialisation has increased by 50% in the past decade. In 2017, there were even some unfilled training posts. This initiated an international marketing campaign, targeting Irish and other European graduates of medical schools in Australia, Canada, and New Zealand, which also resulted in successful applications from a number of international medical graduates working in non-training posts in Irish hospitals.
4.6. Conclusions
The current situation in medical education and workforce in Ireland is very paradoxical: Irish medical schools are providing education to a very large number of Irish and international students, yet Ireland is heavily dependent on the recruitment of foreign-trained doctors. This is due to the fact that most international graduates of Irish medical schools cannot pursue their internship and postgraduate training in Ireland after they get their first medical degree and many Irish graduates and doctors also move abroad to obtain better training and job opportunities. This paradox reflects at least two issues of policy coherence: 1) between the initial medical education programmes and the next steps in the training of doctors which include an internship and postgraduate training programmes; 2) between the education of doctors and recruitment and retention policies.
Sooner or later, the lack of access to internships in Ireland for most international graduates of Irish medical schools is likely to have an impact on the schools’ international reputation and reduce their attractiveness – and by that their funding and ability to provide a high-quality education –, unless these international graduates are able to find sufficiently good opportunities for finishing their medical education in their own country or in a third country. It has become increasingly difficult, for example, for the growing number of Canadian students who complete their first medical degree in Ireland to find a residency placements in Canada, as majority of the available residency positions are earmarked for the medical graduates trained in Canada (CaRMS, 2019[32]). Finding a way for non-EU/EFTA graduates of the Irish medical schools to do the internship year and obtain the right to practice in Ireland could also be a response to the domestic needs for doctors.
Another concern is the lack of access to specialist training for a high number of foreign-trained junior doctors working as NCHDs in Ireland: this bears a risk of de-skilling and could ultimately affect the quality of health care services in Ireland. Moreover, considering the World Health Organization (WHO) Global Code of Practice on the International Recruitment of Health Personnel, Ireland should strive to meet its commitments under the Code’s aims of reducing the need to recruit migrant doctors and of offering equal employment opportunities to those doctors once they were working in Ireland.
Considering the number of interconnected issues that need to be addressed – ranging from the desired level of internationalisation in medical education and training to the availability and quality of internship and postgraduate training places as well as the working conditions in the Irish Health Service – it is necessary to establish effective coordination mechanisms between the various actors in the medical education and health employment sector. There is, however, limited interaction and engagement between the various bodies involved in medical education, postgraduate training, and health employment. In particular, there is no forum for discussion of challenges relating to the internationalisation of medical education.
In fact, the lack of dialogue between the medical education and health sectors was mentioned by representatives of the Department of Health, who referenced the 2017 National Strategic Framework for Health and Social Care Workforce Planning as a starting point for this dialogue (Department of Health, 2017[33]). Under this framework, the Department intends to develop a protocol for engagement between the health and education sectors. Key actions will include establishing governance and oversight structures for workforce planning, building communications and engagement between stakeholders, developing protocols for the engagement between the education and health sectors, and expanding the evidence base. The implementation of these actions is ongoing. A new Health Workforce Planning Unit within the HSE is also being established under this framework, with the support of the NDTP (responsible for postgraduate training).
Similar actions and coordination efforts had already been proposed in the 2006 Fottrell Report (Department of Health, 2006[9]), but were not followed up by actual implementation. Other policy documents – such as the 2014 Department of Health review (also referred to as the MacCraith Report) – also have not led to any meaningful policy implementation. The 2014 review noted, for example, the issues with junior doctors in non-training posts and made recommendations to improve the situation (Department of Health, 2014[34]); but a seventh progress report on this review from June 2018 stated that there had been no significant progress on this issue, aside from a commitment to carry out another review (Department of Health, 2018[35]).
In general, a number of key questions remain to be addressed:
-
Is it desirable to have a large number of international students enrolled in a first medical degree if most of them will not have the opportunity to complete their education and training in Ireland? On the one hand, Irish medical schools are contributing to the international pool of medical graduates available to pursue their postgraduate training, but if these new medical graduates cannot find internship or specialist training places anywhere – in Ireland, at home, or a third country –, this might result in a “brain waste” (waste of human capital). Where is the balance and how can state funding of medical education help to strike this balance?
-
As is obvious from the large number of foreign-trained foreign-born doctors currently working in the country, Ireland has a significant need for doctors beyond its native-born native-trained graduates. Hence, why not plan to retain some of the international graduates of Irish medical schools, who are already acquainted with the Irish health system?
-
Is there a way to increase the number of internship places without compromising the quality of the training to give greater opportunities for international students to complete their medical education and training in Ireland?
-
How can foreign-trained doctors be offered better access to specialist training?
These concerns about the current situation in medical education and training and the related implications for the medical labour market are well recognised and shared among key policy stakeholders in Ireland, yet the implementation of policy actions to address these issues continues to lag.
References
[12] Atlantic Bridge (2018), Atlantic Bridge, https://www.atlanticbridge.com/medicine/ (accessed on 13 November 2018).
[23] Brugha, R., F. Cronin and N. Clarke (2018), Retaining our Doctors. Medical Workforce Evidence 2013-2018, Royal College of Surgeons in Ireland.
[8] Campbell, T. (2015), Medical Workforce Analysis: Ireland and the European Union compared, Department of Public Expenditure and Reform (DPER).
[32] CaRMS (2019), Canadian Resident Matching Service, https://www.carms.ca/match/r-1-main-residency-match/ (accessed on 5 July 2019).
[11] Central Applications Office (2018b), Graduate Entry Programmes in Medicine – Ireland, http://www2.cao.ie/downloads/documents/2019/GraduateEntryMedicine2019.pdf (accessed on 10 December 2018).
[10] Central Applications Office (2018a), Selection criteria for undergraduate entry to medicine for EU applicants 2019, http://www2.cao.ie/downloads/documents/2017/UGMedEntry2017_ir.pdf (accessed on 10 December 2018).
[35] Department of Health (2018), MacCraith 7th progress report, Department of Health, https://health.gov.ie/wp-content/uploads/2018/07/MacCraith-IMG.-Seventh-Report.-12..pdf.
[33] Department of Health (2017), Working Together for Health- A National Strategic Framework for Health and Social Care Workforce Planning, Department of Health.
[34] Department of Health (2014), Strategic Review of Medical Training and Career Structures Report on Medical Career Structures and Pathways following completion of Specialist Training (MacCraith Report), Department of Health, https://health.gov.ie/wp-content/uploads/2014/04/SRMTC.
[9] Department of Health (2006), Medical Education in Ireland: A New Direction, Dublin.
[19] Government of Ireland (2011), Government of Ireland Student Support Act, http://www.irishstatutebook.ie/eli/2011/act/4/enacted/en/html.
[18] Haugh, C., B. Doyle and S. O’Flynn (2014), “Debt Crisis ahead for Irish medical students”, Irish Medical Journal, Vol. 107/6, pp. 185-6.
[7] Health Education Authority (2018b), HEA (2006-2016) student data, http://hea.ie/statistics-archiv (accessed on 10 November 2018).
[3] Health Education Authority (2018b), Health Education Authority, http://hea.ie/funding-governance-performance/funding/student-finance/course-fees/ (accessed on 13 November 2018).
[2] Health Education Authority (2018a), http://hea.ie/statistics-archive/, http://hea.ie/statistics-archive/ (accessed on 11 October 2018).
[5] Health Service Executive (2018), Health Service Executive Medical careers, http://www.medicalcareers.ie/about/specialty-grades/ (accessed on 13 November 2018).
[27] Humphries, N. et al. (2017), “The consequences of Ireland’s culture of medical migration”, Human Resources for Health, Vol. 15/1, https://doi.org/10.1186/s12960-017-0263-7.
[20] Indecon (2005), The Cost of Undergraduate Medical Education and Training in Ireland, Indecon.
[21] Irish Universities Association (2018), Funding Irish Universities to Fuel the Knowledge Economy - Budget 2019 Submission.
[13] IUMC (2018), IUMC, http://www.iumc.com.my/Aboutus.php (accessed on 13 November 2018).
[6] Medical Council (2013), Medical Education, Training and Practice in Ireland 2008-2013 A Progress Report, Medical Council, https://doi.org/www.medicalcouncil.ie/News-and-Publications/.
[31] Medical Council Annual report 2017 (2018), Medical Council Annual report 2017, Medical Council, https://www.medicalcouncil.ie/News-and-Publications/Reports/Annual-Report-2017.pdf.
[24] NDTP (2018), NDTP, https://www.hse.ie/eng/staff/leadership-education-development/met/ed/img/ (accessed on 13 November 2018).
[4] NDTP (2017), National Doctors Training and Planning: Annual report 2016, Health Service Executive, https://www.hse.ie/eng/staff/leadership-education-development/met/publications/ndtp-annual-report-2016.pdf.
[29] NDTP (2018b), Eighth annual assessment of NCHD posts 2017-2018, Health Service Executive.
[16] NUIG (2018), NUIG Galway, https://www.nuigalway.ie/student-fees/pay-fees/ (accessed on 13 November 2018).
[26] OECD (2019), “Health workforce migration”, OECD Health Statistics (database), https://dx.doi.org/10.1787/1497601f-en (accessed on 26 June 2019).
[1] OECD (2018), Education at a Glance 2018: OECD Indicators, OECD Publishing, Paris, https://dx.doi.org/10.1787/eag-2018-en.
[28] Public Service Pay Commission (2018), Report of the Public Service Pay Commission: Recruitment and Retention Module 1, https://paycommission.gov.ie/wp-content/uploads/pspc-report-2018-body_web.pdf.
[30] RCPI (2017), National Study of Wellbeing of Hospital Doctors In Ireland. RCPI, Royal College of Surgeons in Ireland.
[17] RCSI (2018), RCSI, medicine fees and funding, https://www.rcsi.com/dublin/undergraduate/medicine/fees-and-funding (accessed on 13 November 2018).
[22] RCSI (2018b), RCSI International, http://www.rcsi.ie/international (accessed on 13 November 2018).
[15] Student Universal Support Ireland (2018), Student Universal Support Ireland, https://susi.ie/undergraduate-income-threshold-and-grant-award-rates/ (accessed on 13 November 2018).
[14] UCD (2018), UCD, http://www.ucd.ie/medicine/news/september2015/title,251666,en.html (accessed on 14 November 2018).
[25] Walsh, A. and R. Brugha (2017), Brain Drain to Brain Gain: Ireland’s Two-Way Flow of Doctors, Royal College of Surgeons in Ireland.
Notes
← 1. Authors’ analysis of HEA’s statistics archive student data for 2006-2016, 8 November 2018: http://hea.ie/statistics-archive/.
← 2. The first year of the six-year programme is a foundation year, from which some students may be exempt depending on their academic qualifications. At the Royal College of Surgeons in Ireland, for example, the foundation year programme aims to develop the English language proficiency of students coming from countries where English is not the first language. The National University of Ireland, Galway offers a foundation year for students who did not take physics, chemistry or biology.
← 3. While there is no specific cap on the number of non-EU/EFTA students, it is within the remit of the Medical Council to inspect medical schools and to ensure that they possess the capacity for the overall number of students within the school.
← 4. Because of its independent status, the Royal College of Surgeons in Ireland receives only the HEA grant in lieu of undergraduate fees, not the HEA block grant.
← 5. NCHDs are medical graduates who have not yet completed specialist training.
← 6. The current intern-matching procedure prioritises those graduates of Irish medical schools who entered these schools through the Irish State’s Central Applications Office (CAO) admissions system, the majority of whom are Irish nationals. As a rule, foreign candidates enter the medical schools through separate channels (see also Box 1.2 and Box 4.2).
← 7. The report notes difficulties in establishing the exact number of vacant posts.