
Child and adolescent health
Childhood and adolescence are fundamental phases in human development, when young people develop knowledge and skills to deal with critical aspects of their health, and are also the period during which many mental health problems first emerge. The COVID-19 crisis has significantly disrupted children and adolescents’ daily lives, and makes attention to young peoples’ health all the more critical (see Chapter 1 on resilience to the COVID-19 pandemic).
Across EU countries in 2018, about one in three 11-year-old girls and less than one in three 11-year-old boys experienced multiple health complaints, such as feeling “low” or irritable, or experiencing headaches, stomach aches or backaches, or having difficulties falling asleep (Figure 3.18). Some of the physical health complaints that adolescents experience, such as stomach ache or headache, can also be signs of psychological distress. In contrast, over one in two 15-year-old girls reported multiple health complaints, a difference of over 20 percentage points compared to 11-year-old girls. The rates of 11-year-olds and 15-year-olds reporting multiple health complaints are highest among boys and girls in Italy, Bulgaria and Malta.
Mental health problems can be associated with major risk factors, such as heavy episodic drinking, tobacco or illicit drug use, unhealthy nutrition and lack of physical activity (see Chapter 4). Behavioural risk factors such as excessive drinking or drug use can both worsen adolescents’ mental health, and be used as a coping mechanism in the absence of more effective mental health support, as well as contributing to lasting effects on physical health across the life course (e.g. circulatory diseases and some cancers).
Mental health problems and psychological distress are one important driver of suicide among adolescents. Over 1 000 15-19 year-olds died of suicide across EU countries in 2017, and most of these deaths were among boys. Despite the relatively low absolute number of suicides among adolescents, suicide is one of the leading causes of death in this age group. Young people are more likely to attempt suicide if they have a family history of alcohol and drug abuse disorders, have access to firearms, and experience difficult life events at school or at home (McLoughlin, Gould and Malone, 2015). The number of death by suicide among teenagers has decreased by over one-third on average across EU countries between 2000 and 2017.
In recent years (2015-17), the suicide rate among teenagers was highest in Lithuania and Estonia, with rates of over 11 deaths per 100 000 15-19 year-olds, a rate more than 2.5 times higher than the EU average. The lowest rates are reported in Southern European countries (Greece, Portugal, Cyprus, Italy and Spain). Suicide rates among boys was 2.5 times higher than among girls on average across EU countries (Figure 3.19).
Countries have taken steps to support vulnerable adolescents with mental health problems (McDaid et al., 2017; OECD, 2015). Inter-sectoral strategies encompassing health, education and welfare policies can promote and protect the health and wellbeing of adolescents. School-based mental health programmes have been introduced in many countries and can improve social and educational outcomes. For example, the Youth Aware of Mental Health (YAM) programme is in place in ten European countries and is associated with a 55% reduction in suicide attempts and 50% fewer cases of suicidal ideation after 12 months (Wasserman et al., 2015).
The indicator on multiple health complaints is based on the following symptoms experienced in the last six months: headache; stomach ache; backache; feeling low; feeling irritable or bad tempered; feeling nervous; difficulties in getting to sleep; and feeling dizzy. Differences across countries may reflect a different understanding and interpretation of the questions.
Data on multiple health complaints come from the Health Behaviour in School-aged Children (HBSC) study. The HBSC surveys have been undertaken every four years since 1993-94 and now include all EU countries except Cyprus. Data are drawn from school-based samples of 1 500 children in three age groups (11-, 13- and 15-year-olds) in most countries, ensuring that the sample is representative of each age group.
Data on suicide rates come from the Eurostat Database. The registration of suicide is a complex procedure, affected by factors such as how intent is ascertained, responsibility for completing the death certificate, and cultural dimensions including stigma. Caution is therefore needed when comparing suicide rates.
References
Inchley J et al. (2020), Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report, Vol. 2, Key data, Copenhagen: WHO Regional Office for Europe.
McDaid, D., E. Hewlett and A. Park (2017), “Understanding effective approaches to promoting mental health and preventing mental illness”, OECD Health Working Papers, No. 97, OECD Publishing, Paris, https://doi.org/10.1787/bc364fb2-en.
McLoughlin, A., M. Gould and K. Malone (2015), “Global trends in teenage suicide: 2003-14”, QJM, Vol. 108/10, https://doi.org/10.1093/qjmed/hcv026.
OECD (2015), Fit Mind, Fit Job: From Evidence to Practice in Mental Health and Work, Mental Health and Work, OECD Publishing, Paris, https://doi.org/10.1787/9789264228283-en.
Wasserman, D et al. (2015), “School-based suicide prevention programmes: The Seyle cluster-randomised, controlled trial”, The Lancet, Vol. 9/977, pp. 385.
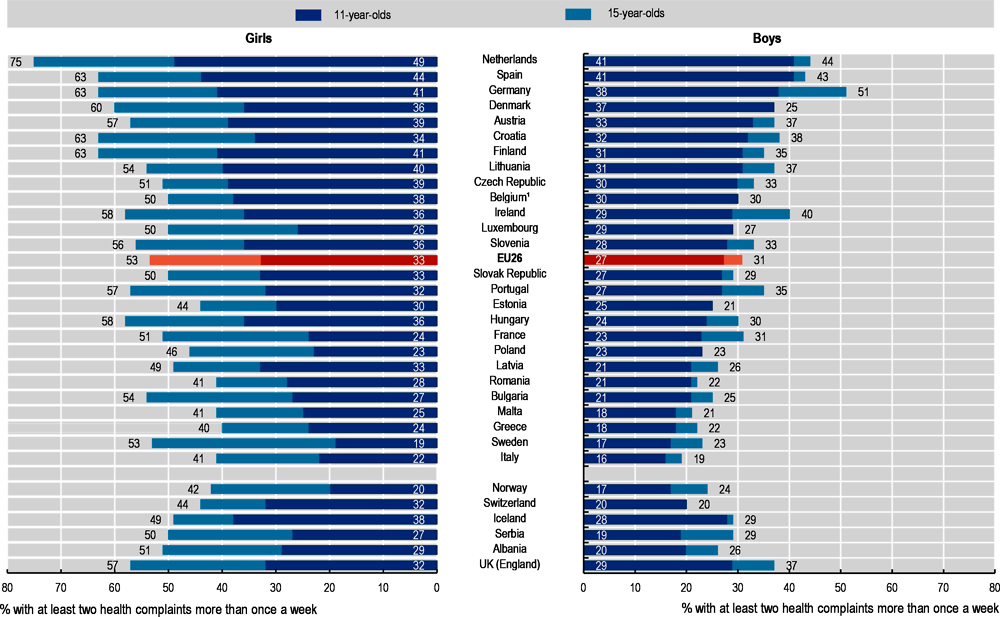
Note: Differences across countries, and especially in Italy, may reflect a different understanding and interpretation of the questions. The EU average is unweighted. The rate for 11-year-old boys is higher than the rate for the 15-year-olds in Romania, Austria and Lithuania. 1. Belgium is the unweighted average of the Flanders region and the French region.
Source: HBSC data from Inchley et al. (2020).
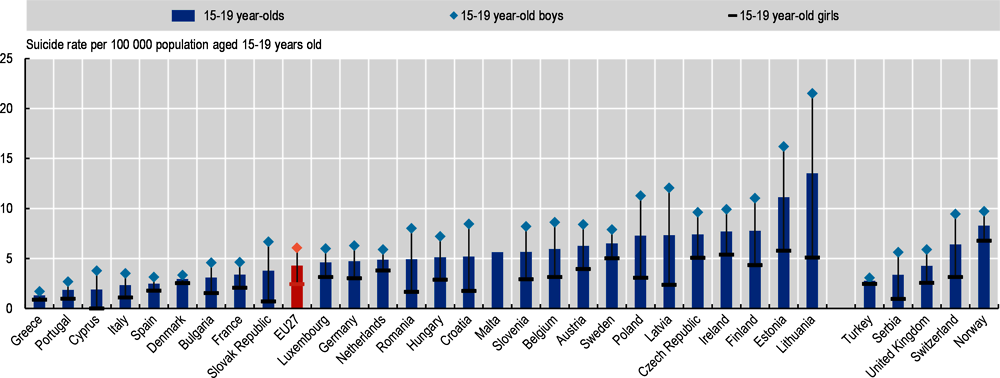
Note: Differences across countries may reflect, at least in part, differences in recording practices. The EU average is weighted. Data refer to a 3-year average (2015-17), except in Cyprus (2015), France (2014-16) and Luxembourg (2014 and 2016 due to missing data in 2015 and 2017).
Source: Eurostat Database.