
Health expenditure per capita
The level of health spending in a country and how this changes over time is dependent on a wide range of demographic, social and economic factors, as well as the financing arrangements and organisational structure of the health system itself.
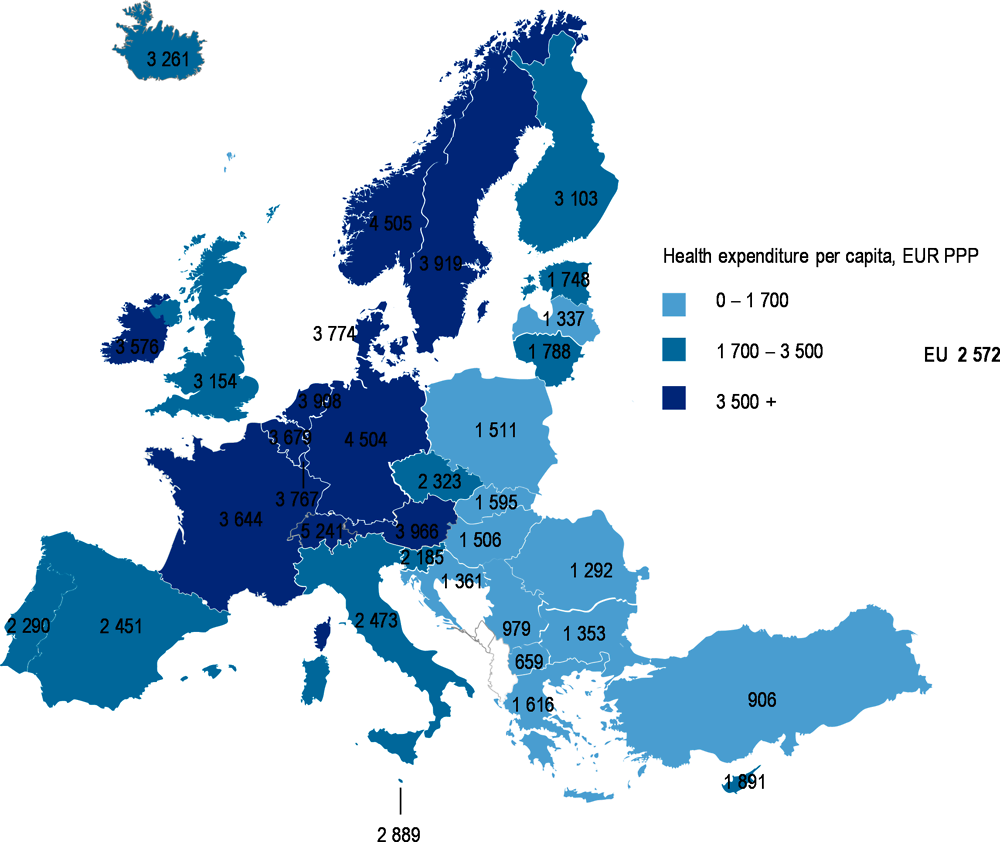
Given these factors, there are large variations in the level and growth of health spending across Europe. There is a strong correlation between income and spending on health, such that high-income European countries are typically those that spent the most on health. With spending at EUR 5 241 per person – adjusted for differences in countries’ purchasing powers – Switzerland was the biggest spender in Europe followed by Norway (EUR 4 505). Among EU member states, spending levels in Germany, Austria, Sweden and the Netherlands were all at least 50% above the EU average (EUR 2 572). At the other end of the scale, Romania, Latvia, Bulgaria and Croatia were the lowest spending countries in the EU, only at around half the EU average (Figure 5.1). This means that on a per capita basis (and after adjusting for differences in price levels), there is a three-fold difference in health spending between high-income countries in Western and Northern Europe and some low spending countries in Central and Eastern Europe.
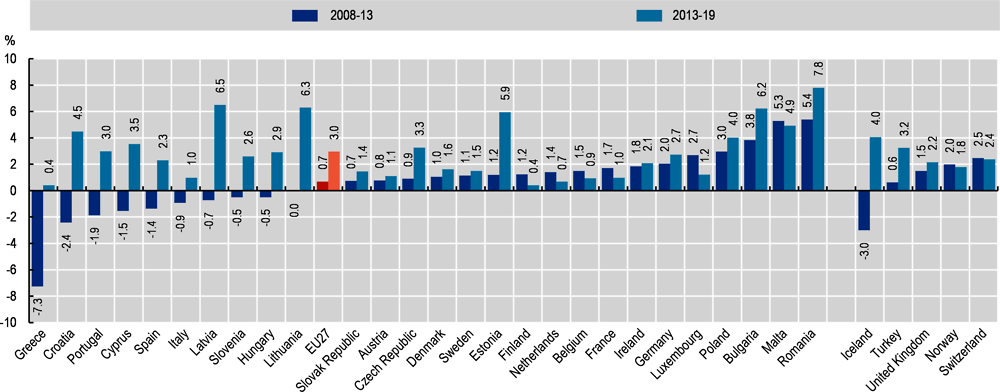
After a period of slow or even negative growth in health spending across Europe in the wake of the economic crisis in 2008, growth rates picked up again in nearly all countries. On average across EU countries, health spending per capita increased by around 3.0% each year in real terms (adjusted for inflation) between 2013 and 2019, compared with an annual growth rate of only 0.7% between 2008 and 2013. All EU countries saw positive growth in health spending between 2013 and 2019, although it remained slow in some countries (Figure 5.2).
Some Central and Eastern European member states with relatively low spending levels like Bulgaria, Romania, Latvia, Lithuania and Estonia, had some of the highest growth rates in health spending since 2013, with annual increases of around 6% or more. In Belgium, Finland, France and the Netherlands, annual per capita health spending growth over the same six-year period remained positive but at around 1% or below and the growth rates were lower than those seen during the years following the 2008 financial crisis. Both Norway and Switzerland maintained a relatively stable rate of health spending growth over the last ten years or so at around 2-2.5% per annum.
Health spending in 2020 across Europe will be significantly affected by the COVID-19 pandemic. The development of the crisis has seen the need for the rapid deployment of resources across the health sector – building up testing and diagnostic capabilities, and providing increased capacity for treatment of patients in the hospital sector. In some countries, health providers received substantial subsidies in exchange for reserving treatment capacity for COVID-19 patients. On the other hand, many countries have seen sharp reductions in many non-COVID related services, such as primary health care consultations and elective surgeries, potentially reducing health care costs for these services. Which of these two opposing trends will dominate in a country is unclear at the time of writing and will depend on many different factors. Chapter 1 provides further information on the budgetary measures that governments have taken to strengthen the health system responses to the coronavirus crisis.
Expenditure on health, as defined in the System of Health Accounts (OECD, Eurostat and WHO, 2017), measures the final consumption of health goods and services. This refers to current spending on medical services and goods, public health and prevention programmes, and overall administration of health care provision and financing irrespective of the type of financing arrangement. Subsidies paid to health care providers should also be included in the figures.
Under Commission Regulation 2015/359, all EU countries are obliged to produce health expenditure data according to the definitions of the System of Health Accounts. Data on health expenditure for 2019 are considered preliminary, either estimated by national authorities or projected by the OECD Secretariat, and are therefore subject to revision.
Countries’ health expenditures are converted into a common currency (Euro) and are adjusted to take account of the different purchasing power of the national currencies, in order to compare spending levels. Economy-wide Actual Individual Consumption (AIC) PPPs are used to compare relative expenditure on health in relation to the rest of the economy.
For the calculation of growth rates in real terms, economy-wide AIC deflators are used. Although some countries (e.g. France and Norway) produce their own health-specific deflators, based on national methodologies, these are not currently used due to the limited availability and comparability for all countries.
For countries where breaks in the time series exist, growth rates are estimated by the OECD Secretariat.
References
OECD/Eurostat/WHO (2017), A System of Health Accounts 2011: Revised edition, OECD Publishing, Paris, https://doi.org/10.1787/9789264270985-en.
Note: The EU average is unweighted. Growth rates and time periods may have been adjusted by the OECD Secretariat to take account of breaks in series.
Sources: OECD Health Statistics 2020; Eurostat Database.