
copy the linklink copied!4. Korea’s preparedness for public health emergencies
Recent disasters and infectious diseases outbreaks have led Korea to reconsider the importance of its preparedness for public health emergencies. This chapter looks at how Korea sets-up and implements public health emergency policies and at how it builds the resilience of its health system, in accordance with the OECD Recommendation on the Governance of Critical Risks and other international guidelines. The chapter suggests that despite the usefulness of policy reforms and new capabilities, strengthening emergency preparedness in Korea remains an unfinished agenda, and more work is needed to address some key areas of weakness.
copy the linklink copied!Introduction
Given the fundamental responsibilities of governments to provide security and safety, citizens and businesses expect them to be prepared for a wide range of possible crises and global shocks, and to handle them effectively should they arise. The first demand on government is to protect citizens’ physical integrity when shock events disrupt the normal functioning of a society. Public health systems play here an essential role in reducing human casualties and other negative health impacts of emergencies, through well-planned and resourced emergency preparedness, and by building resilience to shock events.
While known as the land of the morning calm, Korea regularly suffers contingencies that can have serious public health consequences. In addition to the yearly typhoon season, the last decade has seen a series of large-scale fires, marine and industrial accidents, natural hazards and infectious disease outbreaks affecting Korea. The diversity of these events demonstrates that one cannot adopt a single risk approach when it comes to developing public health emergency preparedness and response capacities or building resilience.
An all-hazards and threats approach to risk management is what the OECD calls for, with its Recommendation on the Governance of Critical Risks, adopted at its Ministerial Council Meeting in 2014. This approach requires working across sectors, though a whole-of-government strategic approach to manage critical risks, which should encompass the different stages of the risk management cycle, from risk assessment, to risk prevention, emergency preparedness and response, and recovery. Engaging the whole-of-society in developing its own resilience is also a critical aspect of modern risk management policies, from local governments to civil society and the private sector.
These principles are well aligned with the International Health Regulations of the World Health Organisation (WHO) regarding preparedness for pandemic and infectious diseases outbreaks, and their three-pronged approach: prevent-detect-respond. They are also consistent with the Sendai Framework for Disaster Risk Reduction adopted in 2015 by the United Nations, which includes preparedness for public health emergencies and health systems resilience amongst its priorities.
With a focus on risk governance, this chapter will assess Korea’s policies and their implementation to prepare for public health emergencies, including but not limited to epidemic and infectious disease outbreaks, floods, earthquakes and other natural hazards, major accidents, as well as security risks. The chapter will focus on how public health emergency stakeholders work jointly across siloes to assess, prepare, detect, respond, recover and learn from public health emergencies. It will also analyse how Korea is building the resilience of its health systems to the diversity of shock events that can occur in our increasingly complex and interconnected societies.
This review was carried out before the start of the outbreak of the coronavirus COVID-19. The COVID-19 outbreak started at the end of the 2019 in China, and rapidly spread to neighbouring countries and across the globe. As of early March 2020, almost all OECD countries report active cases of coronavirus COVID-19.
Korea and other OECD countries are implementing policy actions to contain and mitigate the impact of this global health threat.
copy the linklink copied!4.1. Korea’s risk profile and potential public health consequences
Prior to diving into policies, this section aims at scanning the risk profile of Korea, to evaluate its risk level with respect to public health emergencies and gain insights on why emergency preparedness should be placed at the top of the public health policy agenda in. With a classic risk assessment approach, this section includes information on past emergencies, exposure to hazards and factors of present and future vulnerabilities in Korea.
4.1.1. Preparedness for public health emergencies should be at the top of the policy agenda in Korea
When compared to other OECD countries, Korea’s risk profile shows a moderate risk exposure, in terms of number of disaster events affecting the country every year, pretty close to the OECD average over the last 3 decades (Figure 4.1). However, data on the socio-economic consequences caused by disasters originating from natural hazards, technological accidents, epidemics or acts of terrorism, shows that Korea ranks better at reducing their economic losses than at limiting the number of fatalities they can generate. Out of 38 countries, Korea ranks 22nd in terms of the average economic damages caused by disasters on its GDP (Figure 4.2), but it is the eighth OECD country in terms of number of fatalities caused by disasters on its population (Figure 4.3). There is scope for further progress in Korea to reduce public health consequences of disasters, implying a need to make public health emergency preparedness a priority in the country.
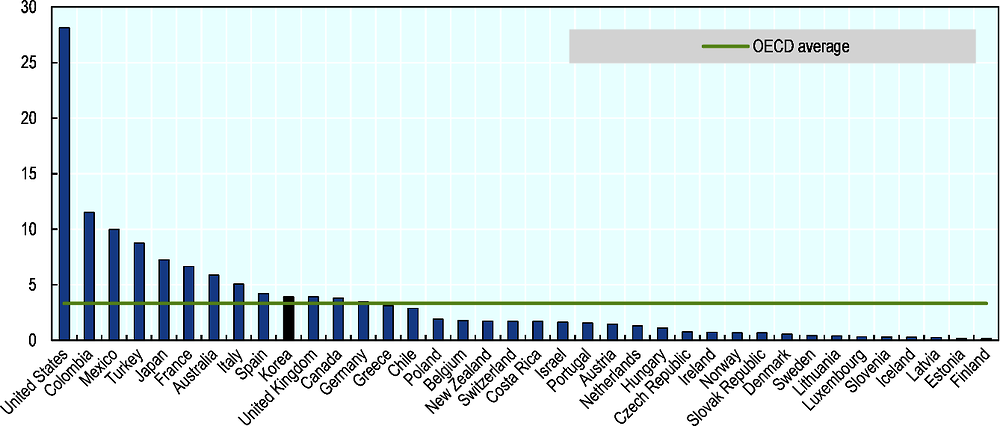
Source: OECD (2018[1]), Assessing global progress in the governance of critical risks, calculation made using data from EM-DAT (2017), International Disaster Database, www.emdat.be and Global Terrorism Database, https://www/start.umd.edu/gtd.
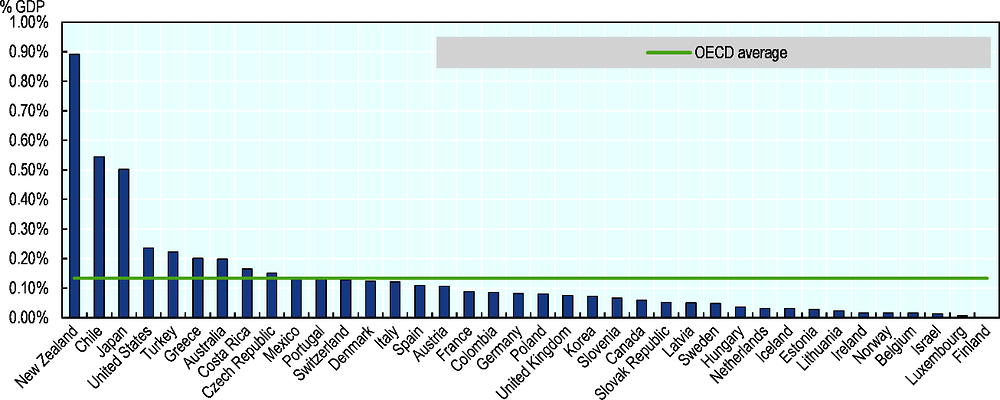
Source: OECD (2018[1]) Assessing global progress in the governance of critical risks, calculation made using data from EM-DAT (2017), International Disaster Database, www.emdat.be, Global Terrorism Database, https://www/start.umd.edu/gtd, and OECD (2017), “Gross Domestic Product” (indicator), https://doi.org/10.1787/dc2f7aec-en.
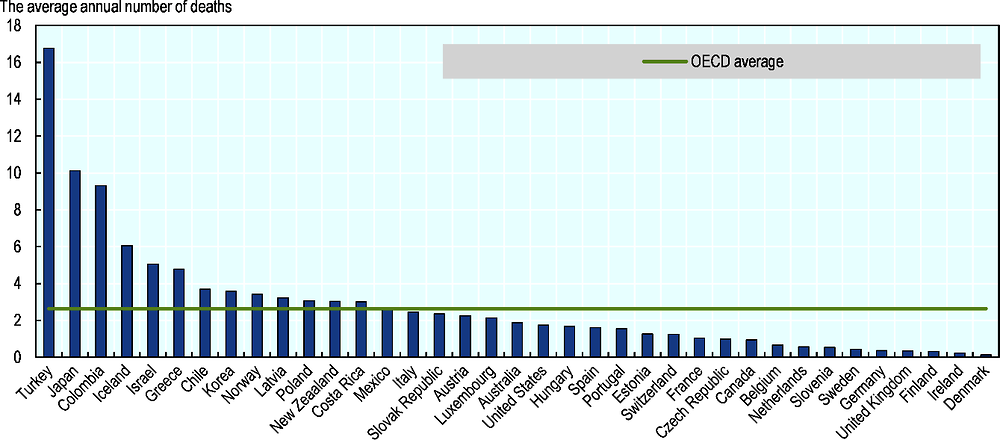
Note: this dataset excludes deaths caused by heatwaves, due to inconsistent reporting of related fatalities across OECD countries.
Source: OECD (2018[1]), Assessing global progress in the governance of critical risks, calculation made using data from EM-DAT (2017), the International Disaster Database, www.emdat.be, Global Terrorism Database, https://www/start.umd.edu/gtd.
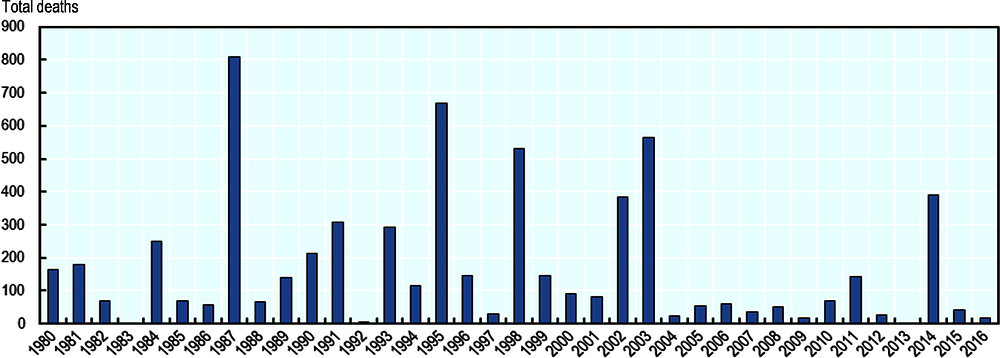
Source: EM-DAT (2017), The International Disasters Database, available at: https://www.emdat.be/.
Recent major crises, such as the Sewol ferry disaster in 2014 or the Middle-East Respiratory Syndrome Coronavirus (MERS-CoV) epidemic outbreak in 2015 revealed major shortcomings in applying safety regulations and managing complex crises, causing significant human losses and large disarray within Korea society (Box 4.1). Recent OECD work on the drivers of trust in public institutions in Korea highlights how the failures in managing these disaster events contributed to lowering the level of trust in the government (OECD, 2018[1]). This has implication well beyond public health, and can affect the overall capacity of the government to function properly and deliver services to citizens. Given persistent low levels of trust in public institution in the country, improving public health emergency preparedness should be seen as a strategic investment for both better health outcomes and reinforcing public trust.
2014 sinking of Sewol ferry: The South Korean ship MV Sewol sinking in April 2014 led to the death of ferry 304 passengers, mostly high school students. It eventually became clear that the accident was caused by over-loading, crating failure and poor initial emergency responses by the crew, coast guard, and Control Center. There was also criticism of the government’s handling of the incident’s aftermath; when government is perceived as failing to handle critical crisis effectively, citizens can come to lose faith in government institutions (OECD/KDI, 2018[2]).
2015 outbreak of Middle East Respiratory Syndrome (MERS): Between May and July 2015 an outbreak of the Middle East Respiratory Syndrome affected 186 people in South Korea, and caused 38 deaths and 16 693 quarantined or isolated individuals. The government, in particular the Ministry of Health (MoH), was heavily criticised for not disclosing relevant information to hospitals and citizens (Reuters, 2015[3]; OECD/KDI, 2018[2]). The MoH did not initially reveal the names of the medical institutions hospitalising the MERS patients, which, according to the MoH’s statement at the time, was intended to avoid unnecessary anxiety to health care users. A number of medical institutions were also criticised; for example in Seoul, 35 infected patients were discharged without knowing that they were infected and allowed to move freely through the city.
Source: OECD/KDI (2018[2]), Understanding the Drivers of Trust in Government Institutions in Korea, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264308992-en; Reuters (2015[3]), “South Korea replaces health minister criticized over MERS outbreak - Reuters”, https://www.reuters.com/article/us-health-mers-southkorea-idUSKCN0Q90JJ20150804
4.1.2. Korea is exposed to natural hazards and climate change calls for elevating public health emergency preparedness for these risks
Natural hazards occur frequently in Korea, which is exposed to floods, typhoons, winter storms, landslides, earthquakes, extreme temperatures and dust storms. While floods and typhoons are the most significant in terms of their frequency and recorded death toll, other hazards such as heatwaves and yellow dust can have also important public health consequences.
Floods and typhoons occur every year in Korea, especially during the summer months, and the associated torrential rains can cause significant socio-economic damage. These hydro-meteorological hazards represented 50% of the disaster events collected in the EM-DAT database over the 1980-2016 period, 50% of the human fatalities and 90 % of both the affected or injured people by disasters and their economic costs (EM-DAT, 2017[4]). Flash floods can be particularly damaging, especially also when they trigger landslides, such as in July 2011, when Seoul metropolitan area was slashed with heavy downpours, resulting in 69 losses of lives and tens of thousands of citizens affected and in need (Reuters, 2011[5]; Asia Sentinel, 2012[6]).
During the typhoon season between June and October, tropical cyclones originating usually east of the Philippines frequently travel towards the Korean peninsula. Typhoons Rusa in 2002 and Typhoon Maemi in 2003 hit the records, being the most powerful cyclones affecting Korea in decades, with strong wind gusts and heavy rains, causing more than 100 deaths each. The most powerful recent typhoon named Bolaven in 2012 also hit the country, with important electricity cuts, large citizen’s evacuations, and 20 human casualties (Table 4.1).
Geological hazards should not be overlooked. While not being as exposed to earthquakes or tsunamis as neighbouring Japan, in 2016 Korea experienced the most powerful earthquakes since the country started recording seismic data in 1978 (Lee et al., 2018[7]), with a second powerful earthquake hitting Pohang city in 2017. North Gygeongsang province was hit these two times, which resulted in 23 injuries, and 9 000 incidents of property damages in the 5.8 magnitude earthquake of 2016 (Korea Meteorological Administration, 2017[8]), and 135 injuries and 1 797 people left homeless in the city of Pohang in the 2017 5.4 magnitude earthquake (Korea Meteorological Administration, 2018[9]).
Both direct and indirect public health consequences of disasters have to be considered: disaster risks, especially large-scale ones, can lead to a significant number of injured people, for whom specific emergency interventions often on-site have to be planned for traumas or burns directly caused by the disaster. From a public health perspective, it is equally important to consider indirect health effects, occurring after the disaster, which can be caused by affected health care provision, post-trauma stress and related psychological impact, or population evacuation and displacement. Large-scale disasters consistently show how damaging these indirect health effects can be. The example of the Great East Japan Earthquakes illustrates the range of consequences (OECD, 2019[10]).
Korea is also exposed to other hydro-meteorological hazards, such as heatwaves and dust storms. While these hazards may appear less destructive, their public health consequences can on the contrary be particularly significant. Recent summers in Korea, for instance, were marked by heatwaves throughout the country, causing excess mortality and significant rises in hospitalisations. The type of health impact caused by heat waves vary greatly, ranging from death, exacerbation of cardiovascular diseases, respiratory diseases, neurological diseases, and psychiatric diseases to the development of heat-related illnesses (Na et al., 2013[11]).
2016 was the hottest year on record since 1972, with 22 heatwaves recorded (Korea Meteorological Administration, 2017[8]). In August 2018, extreme temperatures again broke the records with severe health impacts. According to media sources quoting officials from the Korea Center for Disease Control, the heatwave episode caused at least 42 deaths, and, 3400 people were treated for health-related illnesses, such as heat stroke. This is the highest number of deaths and affected people since South Korea began officially counting casualties due to heat in 2011.
Similarly, yellow dust storm occur regularly in Korea, and can lead to severe public health consequences, such as respiratory diseases (Box 4.2).
Korea is periodically exposed to “yellow dust storms”, which originate in the dry desert regions of China and Mongolia. The storms are driven by low-pressure systems combining with strong winds and cold air fronts, pushing dust into the atmosphere and carrying it across the continent. The impact of this trans-border environmental risk ranges from visibility reduction, to a variety of human health problems, including a negative impact on respiratory function, and a risk of aggravating respiratory diseases such as asthma. Over the past decade, the yellow dust phenomenon has become a more serious problem, because of industrial pollutants and intensified desertification in originating regions. The below table shows yellow dust phenomena that have impacted Korea in the 2003-2012 period; in 2010, there were 15 incidents and a total of 25 days where yellow dust storms were affecting the country The socio-economic impact of yellow dust, stemming from increased medical treatment, decreased industrial and agricultural production, complications in aviation transport and product purchase for preventing the damage, were estimated at 0.8% of Korean GDP in 2002 (Jeong, 2008[12]). Yellow dust storms also have negative effects on water, air, soil and animals.
Climate change and other trends from urbanisation to ageing will affect Korea’s exposure to natural hazards and its vulnerability. According to the Intergovernmental Panel on Climate Change (IPCC) floods and typhoons frequency and strength will be affected, heatwaves are projected to be longer and more intense, and desertification in East Asia might increase the risk of yellow dust storms (Kim, 2017[14]); (Hijioka, Lin and Jacqueline Pereira, 2014[15]).
4.1.3. Korea is at risk of infectious diseases outbreaks and has a high tuberculosis prevalence rate
Regarding infectious diseases outbreaks and the risk of pandemics, Korea, as a global economic hub, is exposed to virus or pathogens in a similar manner to most OECD countries. Korea is also marked by a high prevalence of tuberculosis (TB) and subject to the resurgence of more classic infectious diseases, such as measles, which sporadically continue to affect citizens and cause deaths.
The recent most noticeable examples of outbreaks, such as the MERS-CoV outbreak in 2015, the H1N1 pandemic influenza in 2009 or SARS in 2003 are all revealing of how similar forms of public health emergencies can affect Korea. These outbreaks have shown that Korea is not always best prepared for these emergencies: the SARS epidemic was well handled compared to neighbouring countries, the H1N1 response did show few shortcomings, and many of the MERS-CoV consequences could have been limited with a better response.
As highlighted earlier, the recent Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in 2015 demonstrated significant shortcomings in Korea’s preparedness for public health emergencies. With 186 confirmed cases, 38 deaths and 16 693 quarantined or isolated individuals, Korea has been the most affected country in the world outside of the Middle East from where this virus originated (Ki, 2015[16]). Almost all the infected cases originated the original patient returning from a business trip in the Middle East in May and few other “super-spreaders” that this individual infected. Several studies point out that these nosocomial infections could have been much more limited as the outbreak was not attributable to biomedical factors but rather due to late diagnosis, quarantine failure for super-spreaders, familial care-giving and visiting, poor crisis communication, inadequate hospital infection management, as well as the doctor-shopping habit within Korean society (Kim et al., 2017[17]; Cho et al., 2016[18]). This outbreak brought significant concerns about public health emergency preparedness in Korea.
Like most OECD countries, Korea was affected by the H1N1 pandemic influenza in 2009. From its emergence in March 2009 in Mexico, the first case in Korea was confirmed early May 2009 and another break out in an English Institute happened in late May that same year (Kim et al., 2010[19]). Influenza activity peaked in October reaching 45 cases per 1 000 inhabitants, spreading across local communities, in particular in schools. The epidemic declined rapidly after the vaccination programme started in early November and reached baseline levels in February 2010 (Yun et al., 2017[20]). Between May 2009 and August 2010, there were 750 000 cases of pandemic influenza H1N1 that were confirmed by laboratory tests and the number of H1N1-related deaths was estimated at 252 (Kim, 2016[21]). Data from National Health Insurance Claims database, meanwhile, suggests an overall infection of 3 million Korea residents, and a total cost of the pandemic reaching USD 1.09 billion or 0.14% of the national GDP (Kim, Yoon and Oh, 2013[22]). Korea had a mortality rate of 5.1 deaths per million individuals compared to other OECD countries such as the United Kingdom (2.2), Canada (2.8), Mexico (2.89), United States (3.3), New Zealand (4.4), Chile (8.1), or Australia (8.6), and significantly higher than neighbouring Japan (0.2) (Takahashi et al., 2017[23]).
Other infectious disease outbreaks with global or regional impacts, such as SARS in 2003, which affected many neighbouring Asian countries, or Ebola haemorrhagic fever in 2014, did not affect Korea or only had a limited impact. Korea was the model of disease containment during SARS: only three confirmed cases and no deaths, despite many Koreans living in or travelled to the SARS major epicentres in neighbouring countries (Hong and Collins, 2006[24]). As a comparison, China was significantly affected, with 349 deaths out of more than 5 327 cases (ibid.).
The prevalence or resurgence of other infectious diseases should also be considered. TB in Korea remains a serious health problem with an estimated 77 per 100 000 incidence rate for 2016. This makes Korea the only OECD country with high incidence of TB: for instance, the rate is 3.1 in the United States, 5.5 in Canada, 6.8 in Australia, 8 in France, 8.9 in the United Kingdom or 15 in Japan (World Health Organisation, 2018[25]). According to data from the Korean Center for Disease Control, in recent years there has been a decreasing rate of new cases of TB infection, which had peaked in 2011 to 78.9 per 100 000 inhabitants (Table 4.3), just before the government released its new five-year tuberculosis control plan for 2013–2017 (Go et al., 2018[26]).
4.1.4. Accidents have caused significant public health damages in Korea
Korea also experienced in the last few decades a series of major accidents in different sectors, which led to important public health emergencies. The Sampoong department store collapse in 1995, the Daegu subway fire in 2003, the Gumi chemical leak in 2012, and the Ferry Sewol disaster in 2014, all have had a tragic death toll, with many injured and affected people. Overall industrial accidents, transport accidents, maritime accidents human casualties represent half of the total casualties caused by disasters in Korea, which makes of better preparing for their human consequences a priority.
These disasters require that public health emergency managers better prepare their capacities and plans to respond to mass casualties’ events, toxic chemical leaks or oil spills, maritime disasters, and industrial fires. This is all the more important given the significant shortcomings that these accidents highlighted, such as the delay in deciding to evacuate affected zones by the hydrogen fluoride gas leakage in Gumi in 2012, which affected 12 000 residents with various health symptoms (Bae, Joo and Won, 2015[28]). Coordination failures among the emergency responders were also particularly tragic in the case of the Ferry Sewol sinking, during which 304 passengers, including 250 high-school students, could not be evacuated despite the presence of the emergency responders, and died of drowning (Dostal, Kim and Ringstad, 2015[29]).
These different disaster events tend to show that the implementation of safety regulations in Korea could be improved. Furthermore, with regards to the resilience of the health sector in Korea, it is important to flag that several accidents occurred in recent years in health facilities, such as fires in hospitals or nursing homes, which not only has had significant casualties but can also further affect health service provision.
4.1.5. Rising vulnerabilities call for strengthening public health emergency preparedness in the years to come
In terms of its vulnerabilities to natural hazards, accidents, and infectious diseases, Korea presents some characteristics that are important to consider in order to prepare for future risks as called for by the OECD Recommendation on the Governance of Critical Risks. Korea’s risk profile depends upon a series of factors, such as the ageing population, population density, international exchanges and travels, ageing infrastructure, as well as hygienic precautionary measures taken by the population, population health conditions, vaccination coverage rate (Chapter 1), and levels of anti-microbial resistance. Korea presents a mixed situation when we look at the different indicators related to such vulnerabilities.
Korea’s rapidly ageing population raises concerns for public health emergency preparedness, given the specific vulnerabilities of elderly people. According to the OECD Demography and population Database, population ageing in Korea is projected to be the fastest in the OECD. In 2050, the Korea population over 65 years will represent over 70% of the population aged between 15 and 64, compared to only 20% in 2015 (OECD, 2018[30]). Elderly persons are particularly vulnerable to airborne and respiratory diseases that can be caused by sand and dust storm (UNEP, WMO and UNCCD, 2016[31]), as well as to risks of heatwaves. When flood, typhoons or earthquakes happen, the elderly are also more susceptible to be injured, have more difficulties evacuating and protecting themselves, and can be affected disproportionally by their indirect effects (Aldrich and Benson, 2008[32]; Yoo, Lee and Tullmann, 2016[33]). This holds also true for infectious diseases outbreaks, where poorer health conditions of elderly people can contribute to aggravating health consequences of infections.
Korea’s high population density, and the large and increasing numbers of inbound and outbound travellers to and from the country are factors that can favour the spread of infectious diseases. Indeed, Korea concentrates five of the densest metropolitan areas in the OECD (Figure 4.5). With 14 million visitor arrivals and 26 million Koreans travelling abroad in 2018, Korea more than doubled the number of inbound and outbound travellers in a decade (Korea Tourism Organisation, 2019[34]).

Note: Light grey bars represent metropolitan areas in Korea
Source: OECD (2019[35]), “Metropolitan areas”, OECD Regional Statistics (database), https://dx.doi.org/10.1787/data-00531-en.
As explained in Chapter 1, Korea’s vaccination programmes follows WHO recommendations; vaccinations are highly recommended for 16 selected diseases as routine vaccination and are administered for free through the National Immunization Program (NIP), including TB, polio, and measles. Overall the vaccination rate in Korea slightly exceeds the OECD average contributing to a good level of immunisation for many infectious diseases.
The growing challenge of anti-microbial resistance (AMR) around the world is also a concern for Korea’s preparedness for public health emergencies. Despite the decreasing consumption trends, antibiotic consumption in Korea is relatively high, with 31.7 defined daily doses (DDD) per thousand inhabitants in 2016, compared to the OECD average of 23.7 DDD (OECD, 2018[36]). In addition, the prevalence of the most resistant organisms is increasing significantly as per the results of a Korea nationwide surveillance study reporting high rates of several resistant organisms (Ryu, 2017[37]). Beyond nosocomial infections, this raises concerns on the risk of outbreaks of anti-microbial resistant infections at community levels, for which Korea started to collaborate horizontally with its 5-year National Action Plan, which follows the One Health approach promoted by WHO.
Finally, while difficult to measure, the significant use of precautionary and hygienic measures within the Korean population is largely recognised as a factor that limits the risk of infectious diseases propagation in the country. These measures include regular handwashing and the widespread use of face masks, which has significantly increased amongst the population in recent years, especially following the H1N1 outbreak (Park et al., 2010[38]).
copy the linklink copied!4.2. Korea makes of preparedness for public health emergencies a priority, as reflected in its public policies
In light of major risks for public health, Korea makes of preparedness for public health emergencies a key policy priority. This is first reflected in its legal and institutional framework related to the important risks of pandemic outbreaks and disasters.
4.2.1. Korea’s legal framework for public health emergencies is based on an all-hazard approach
As in many countries, following major crises Korea readjusted its legal and institutional framework to better prepare for public health emergencies.
In 2004 the Framework Act on the Management of Disasters and Safety established a comprehensive system for emergency management in Korea. By addressing both natural and social disasters – which includes infectious diseases – this legislation was the first taking an all-hazard and threat approach to emergency management in Korea, as recommended by the OECD Recommendation on the Governance of Critical Risks. Prior to this act, there were more than 70 disaster-related laws and executive orders under the jurisdiction of 13 different agencies, which created significant governance gaps and coordination challenges (Bae, Joo and Won, 2016[39]). Drawing lessons from the series of disasters which affected Korea in the early 2000 - Typhoon Rusa in 2002, Daegu subway fire in 2003, SARS epidemic in 2003 – the administration designed the Framework Act to streamline government efforts in emergency preparedness and foster whole-of-government coordination.
With the overall aim of protecting citizen’s lives, safety and property, the Framework Act on the Management of Disasters and Safety clarifies the responsibilities of national to local governments all across the risk management cycle, from prevention, to preparedness, response and recovery (Government of Korea, 2015[40]; Heo, Park and Heo, 2018[41]). The Act instructs all levels of government to establish both a Safety Management Committee for policy planning and implementation and a Disaster and Safety Countermeasures Headquarter for operational response, as well as the development of Safety Management Plans in all local governments, aligned with the national Master Plan for Safety Management developed every 5 years.
While the Act states that local governments bear the primary responsibility for emergency response, it also includes a series of provisions for direct interventions from the national level, when local capacities are overwhelmed, when several local governments are affected or in case of declaration of State of Disaster by the Ministry of Interior and Safety. The principles of mutual cooperation should then apply, which can at times create confusion in the response.
The Act promotes a series of emergency preparedness measures, including the development of alert systems, response manuals, and emergency drills, as well as reporting systems on a local safety index, post event reviews, safety inspections and related financing and incentive mechanisms. The Prime Minister, who chairs the Central Safety Management Committee, together with the Ministry of the Interior and Safety, bear the primary responsibility for overseeing policy implementation and ensuring multi-stakeholder coordination.
Regarding infectious disease, the Framework Act was complemented in 2010 by the Infectious Disease Control and Prevention Act in order to reflect the 2005 International Health Regulation adopted at the WHO, as well as the lessons from the H1N1 influenza pandemic. The Infectious Disease Control and Prevention Act first defines categories of infectious diseases depending on their infectiousness and the severity of the symptoms. The Act requests that the Ministry of Health and Welfare prepare the Master Plan for preventing and controlling infectious disease every 5 years and to establish the Infectious Disease Control Committee. It specifies also the responsibilities of the various levels of governments and health institutions for the national infectious disease surveillance and detection system, the vaccination programme, the various infection control countermeasures, the stockpiling policy for medical countermeasures as well as a set of financing and compensation regulations. However, the Act does not specify the coordination mechanism between the various levels of government in great details, which can create governance loopholes during outbreaks, as was the case during the MERS epidemic.
Both the Framework Act on the Management of Disasters and Safety and the Infectious Disease Control and Prevention Act have been updated in recent years to incorporate lessons learned following the 2014 Ferry Sewol accident and the 2015 MERS-CoV outbreak and adjust the institutional framework. These changes addressed some of the most pressing needs identified after these disasters, such as the lack of coordination between emergency response agencies in the first case or the need to strengthen the infectious disease control system, reinforce hospital regulation and increase public health workforce in the second. It remains to be seen whether the fundamental governance challenges of properly articulating local and national responsibilities and resources in public health emergency preparedness (Bae, Joo and Won, 2016[39]) have been effectively addressed.
4.2.2. Korea reformed its institutional setting for public health emergency preparedness in recent years
After a series of institutional changes, the Ministry of the Interior and Safety (MOIS), created in 2017 by the new administration, now regroups the different emergency response capacities under its responsibility. MOIS’ Vice-Minister for Disaster and Safety Management oversees the National Disaster and Safety Control Center for the operational response as well as the different policy design and implementation offices related to public safety, risk prevention, emergency preparedness, response and recovery. This follows the 2014 total reform of the disaster management system, which had initially brought these capacities under the direct responsibility of the Prime Minister, in order to regroup the former National Emergency Management Agency, the Korean Coast Guards, and the National Fire Agency under the same umbrella (Park, 2017[42]). While the 2014 reform helped to strengthen horizontal coordination in emergency preparedness and response, this also weakened the link with local governments traditionally governed from the Ministry of the Interior. With the new governance in place, it is now expected that improvements in vertical coordination between the national and local governments will facilitate the construction of a more effective emergency preparedness and response system in Korea.
Regarding the public health sector, the Ministry of Health and Welfare (MOHW) oversees policy development and implementation both for infectious disease control and for disaster emergency healthcare, in accordance with the two aforementioned legislations. The Korea Center for Disease Control (KCDC) is the main operational agency for infectious disease prevention and control, in charge of risk assessment, disease surveillance, risk communication, field investigation, among others. As for the above, this central government agency has seen its role as the control tower for infectious disease emergency preparedness and response significantly reinforced after the MERS-CoV outbreak, with the creation of new divisions to strengthen event-based surveillance, information collection, risk assessment and emergency operations through the establishment of its public health Emergency Operations Center (EOC) (World Health Organisation, 2017[43]). Regarding other types of disaster, MOHW’s Division for Emergency Healthcare coordinates medical emergency support with MOIS in accordance with the Framework Act on the Management of Disasters and Safety.
In addition to MOIS and MOHW, other line Ministries and national agencies contribute to public health emergency preparedness and response in Korea in their respective areas of responsibilities in line with the whole-of-government approach to emergency preparedness adopted in Korea. This includes for instance the Ministry of the Environment for environmental pollution accidents or yellow dust storm, the Ministry of Agriculture, Food and Rural Affairs for zoonotic diseases or the Ministry of Education for disasters in schools, as well as the various emergency response agencies, technical agencies.
4.2.3. Horizontal and vertical policy coordination for public health emergency preparedness
Korea’s horizontal coordination is facilitated at the strategic level through the Central Safety Management Committee, chaired by the Prime Minister and to which the Government Office for Policy coordination and the National Security Council participate as well. Furthermore, MOIS has established dedicated policy bureaus for specific types of disaster events, which allow the Ministry to coordinate more easily with other Ministries involved. For instance, MOIS’s Public Health Disaster Response Division coordinates closely with the MOHW including through staff exchange, which is good practice. As explained above, it appears that the need to strengthen inter-ministerial coordination for a more effective emergency preparedness and response was taken seriously in Korea in recent years, in accordance with OECD recommendations related to strategic crisis management (OECD, 2015[44]).
At the local level, Korea builds on its three tiered decentralised governance system, with its 17 provinces and metropolitan cities and its 226 municipalities, which all have preparedness responsibilities within their jurisdiction. As decentralisation in Korea was initiated in the mid-1990s, local level responsibilities have progressively been devolved to this level. Since the adoption of the Framework Act on the Management of Disasters and Safety in 2004, local governments have seen these responsibilities increasing, as the Act puts emphasis both on strengthening the central command and control system and on decentralising the first response (Bae, Joo and Won, 2016[39]). Local governments have established disaster management divisions and are required to develop their Safety Management Plan in line with national guidelines and manuals. They can count on local Fire Services, 119 Rescue teams and medical institutions. A bottom up approach with scaling up procedures lets higher levels of government provide complementary emergency support in case of need.
In addition to the multi-hazard and threat Safety Management Plan, regional and local governments are required to prepare a specific plan for infectious disease prevention and control. Such plans outline the roles of local government in the infectious surveillance and detection system in Korea, their prevention responsibilities and the various types of countermeasures to be taken at their level when an infectious disease is detected. The central government along with provincial and local governments implement the infectious disease prevention and control policy, together with the network of the 256 Public Health Centers located across Korea, and medical institutions.
Several public health and emergency management officials expressed that strengthening multi-level coordination is a key area to improve preparedness in Korea now that central level governance has been stabilised. Central authorities have powerful policy levers on local governments, as they control a large part of their budget allocations and human resources through the MOIS, set guidelines and evaluate emergency preparedness and related plans. Nevertheless, clarity of roles and responsibilities between the central and local governments could be improved and coordination mechanisms streamlined in order to make the best of existing local capacities and proximity when emergencies unfold (Bae, Joo and Won, 2016[39]).
copy the linklink copied!4.3. Identifying and assessing public health emergencies risk in Korea
Preparing for public health emergencies requires, first, a good knowledge of the critical risks and their potential public health consequences. With an all-hazard approach, Korea has set up sophisticated systems for risk related data collection and analysis with comprehensive information-sharing platforms in the context of the government 3.0 initiative. The development of these tools reflects the advanced technological development and the importance of government innovation in Korea.
By making risk information widely available, such systems let Korea emergency management system identify and asses critical risks and to communicate them across government, from national to local levels, as well as to citizens. Nevertheless, Korea is less advanced when it comes to utilising this rich information-base to strategically plan its emergency response capabilities through a whole-of-government scenario-based National Risk Assessment. Unlike many OECD countries, Korea does not yet undertake such an assessment (OECD, 2018[13]), which would allow the comparison of all major risks in terms of likelihood and potential impacts, and prioritisation of resources accordingly.
4.3.1. Korea has developed advanced risk analysis tools with a multi-hazard approach
As per the Framework Act on the Management of Disasters and Safety, MOIS collects risk-related data and information for all the disaster risks that can affect Korea. This includes information on both natural hazards and social disasters as defined in the Act (Table 4.4).
All sectoral ministries and agencies are required to report disaster’s data and statistics, which has enabled MOIS to develop a comprehensive database of disaster characteristics over the years for all these disaster types, including on their public health consequences (see Box 4.3). Geospatial data has also been collected on hazards, exposure and vulnerability to support risk analysis, through the network of technical agencies and their information systems. This includes for instance meteorological and geological information from the Korean Meteorological Administration, hydrological information from the Flood Control Offices of the Ministry of Land Infrastructure and Transport, geospatial information on human settlements, population density and so on (Kang, 2016[45]). Furthermore, MOIS monitors information on the available emergency response capabilities from the national to the local levels, which is good practice to assess preparedness levels.
Amidst the increasingly more complex nature of disasters, Korea MOIS has established an integrated Disaster and Safety Information System to support cross-government risk information sharing. This information system has integrated 11 previously existing disaster management systems and information from 16 various ministries. Based on a 3-D geospatial information system (GIS) the system makes available all the data and information necessary to conduct risk assessment at the national and local levels. The System’s web based Disaster Management Portal is accessible to central and local governments to access this information as well as to upload their own information. In addition to risk assessment, the system can also be used during the emergency and recovery phases as a risk communication and collaboration tool, facilitating inter-agency response.
Source: Ministry of the Interior and Safety (2019[46]), Integrated Disaster and Safety Information System, https://www.mois.go.kr/eng/sub/a03/bestPractices1/screen.do; Kang (2016[45]), Disaster Early Warning Services in the Republic of Korea, http://www.safekorea.go.kr/ids
This rich information is made available to the various agencies of Korea emergency response system, from the national to the local levels, through the Disaster Management Portal of the Integrated Disaster and Safety Information System set-up after the 2014 revision of the Act (see Box 4.3). Furthermore, MOIS, with the support of its National Disaster Management Institute (NDMI) has developed a project aimed at calculating Safety Index for all the local governments across the country, with information directly available to citizens through Public Safety Maps (Box 4.4). This open platform helps to strengthen citizen’s risk awareness and contributes to making local government more accountable in risk management decision-making.
The Public Safety Map Service (http://www.safemap.go.kr) is designed to provide various, previously scattered information on maps via the Internet and mobile app in eight categories (crime, traffic, natural disasters, safety for the vulnerable, facilities, industries, public health, and man-made disasters). It also provides an alarm service with real-time information, in the areas near the user’s current location using GPS from mobile devices, as well as the location and contact of public facilities including police stations, fire stations, and emergency facilities such as shelters and hospitals. According to MOIS, 2.7 million Korean citizens have accessed these public safety maps.
In addition, MOIS has compiled various safety statistics to compute local safety indices in seven key areas, i.e. traffic accidents, fires, crimes, safety accidents, suicides, and infectious diseases. These are further classified into one of five levels for each local government and disclosed to the public annually. Local governments can use the Local Safety Diagnosis System and local safety indices to identify local risk factors in their areas for improvement, and the central government offers consulting. Such efforts have resulted in the mitigation of negligent accidents in each area.
Source: Ministry of the Interior and Safety (2019[46]), Integrated Disaster and Safety Information System, https://www.mois.go.kr/eng/sub/a03/bestPractices1/screen.do.
4.3.2. For infectious diseases, KCDC has strengthened its risk assessment process following the MERS-CoV outbreak
Under the Infectious Disease Prevention and Control Act, Korea has established a list of notifiable infectious diseases and defined 11 categories of infectious diseases according to their infectiousness and the severity of the symptoms (Table 4.5). In addition to contributing to the whole-of-government risk assessment process presented in the section above, KCDC monitors and assess these risks using a classic risk assessment methodology combining their likelihood and potential impact. This new risk assessment approach is promising and could be further institutionalised as an element of a wider National Risk Assessment.
The development of this methodology follows a major strengthening of KCDC’s capacities in the aftermath of the MERS-CoV outbreak. In light of the failure to identify key vulnerabilities of the Korean medical system as an important risk factor (Park, 2017[42]), KCDC has reinforced its risk assessment process, notably with the creation of its Risk Assessment & International Cooperation Division. Concretely, criteria have been defined to characterise four different levels of likelihood, and five levels of potential impacts for the different infectious diseases. A matrix analysis then defines five levels of risks (very low, low, moderate, high and very high), the highest level being the most likely with the highest potential impact. Data used in this risk assessment includes yearly domestic cases (by months, cities or province), domestic response capacities (response system, laboratory diagnostics, and supply of vaccines), as well as public perception.
Eleven priority infectious diseases have been identified by KCDC, forming the basis for planning and resource stockpiling (World Health Organisation, 2017[43]). This includes diseases that are candidate for eradication, those identified by WHO as threats to global public health security (smallpox, wild-type Poliomyelitis, new types of Influenza, Pneumonic plague, viral haemorrhagic fevers), MERS and any other infectious diseases with a risk assessment level of moderate to higher.
The development of this risk assessment enables Korea to prioritise the different risks for which it should develop public health response capacities. This aligns well with the purpose of risk assessment as expressed in the OECD Recommendation on the Governance of Critical Risks. It remains nevertheless unclear how this risk assessment corresponds to the categories of infectious diseases enshrined in the Infectious Disease Prevention and Control Act, and whether the results of this risk assessment are shared within the wider whole-of-government risk assessment stakeholders as well as with local governments. For instance, KCDC pandemic influenza scenario is not shared with local governments in details, which is a missed opportunity for them to prepare their planning accordingly.
4.3.3. Korea could further benefit from its advanced risk assessment capacities by developing a National Risk Assessment
As shown in previous sections, Korea has effectively developed databases, information systems and analytical tools that enables national and local governments to conduct risk analysis and base their emergency preparedness and planning on this evidence. The revision of the national governance, which makes MOIS the central national institution for emergency preparedness, and the mandate it has received to develop risk analysis with all the emergency response stakeholders provides a robust base for developing a more ambitious approach with a national risk assessment. In addition, the new risk assessment approach developed by KCDC demonstrates the value of using such analytical tool, which makes it possible to compare the different risk the country faces depending on their likelihood and potential impacts. As expressed in OECD cross country analysis on National Risk Assessments (OECD, 2018[13]), Korea has all the technical ingredients in place for such comprehensive approach, which is in place in a large number of OECD countries such as the Netherlands (Box 4.5).
The benefits of a whole of government approach are numerous and can create an even greater level of protection for citizens. These benefits include optimisation in the allocation of resources in dealing with the most serious risks that have been identified as affecting the country. Additionally this should lead to a reduction in the unpredictability of risks and the identification of the highest risks which may require special treatment by government and experts in this particular subject matter. The adoption of a strategic approach specifically focused on a better strategy for managing risk would provide an objective and systematic evidence base for government-level emergency planners and foster cooperation across government.
A comprehensive national risk assessment could provide crucial support to an effective strategy for the governance of critical risks in Korea. It would draw from existing technical capacities in risk assessment, and provide an overarching framework across different fields of expertise to conduct analyses according to common criteria. This would help to prioritise investments in the mitigation of risks and their consequences and improve overall preparedness and consequence management.
The Netherlands has regularly conducted a National Risk Assessment (NRA) since 2008. The NRA supports development of a cross-government National Safety and Security Strategy, providing an evidence base for determining priorities for risk reduction and prevention, and through investment in capabilities for response to and recovery from civil contingencies. Expertise from the private and academic sectors is strongly integrated into the analytical process supporting the NRA, through the use of a Network of Analysts for National Security. The National Steering Committee for National Safety and Security is the sponsor of the entire exercise. The NRA method is scenario-based.
Risk scenarios are assigned scores for their likelihood and impact on the different national security interests. The results give high and low estimates of a risk occurring. The impact assessment allows the Netherlands to determine which capabilities are needed for each type of risk. Each NRA is reported to parliament accompanied by an account of the capabilities that the government has decided need be reinforced, based on the NRA. For each of the main risks assessed, a capability analysis is carried out under the responsibility of the government department that is most involved, with support from the Ministry of Security and Justice.
Source: OECD (2018[48]), OECD Toolkit on Risk Governance, https://www.oecd.org/governance/toolkit-on-risk-governance/home/.
copy the linklink copied!4.4. Capabilities for public health emergency preparedness and response in Korea
Based on its risk analysis and following recent disaster events, Korea has invested resources for the development of a robust infrastructure and dedicated capabilities to prepare for public health emergencies, from their detection and surveillance to emergency response and medical care. A notable budget increase in risk management contributed to strengthening Korea’s emergency capabilities significantly in the last 5 years, with the creation of new information systems, the enhancement of health care infrastructures, and the reinforcement of human resources, especially for infectious diseases preparedness and control. While progress can be continuously undertaken in this domain, these capacities appear to be generally tailored in good accordance with the level of risk in Korea, national policies and international standards, particularly at the national level. Nevertheless, ensuring that local government also build the commensurate capabilities to properly fulfil their requirements is a concern across health and emergency professionals.
4.4.1. Surveillance, monitoring and information systems make good use of innovation to detect public health emergencies.
Korea has invested significantly in its capacities to monitor, detect, and analyse threats to public health, as well as to warn emergency responders and citizens in case of disaster events. Making the best of the widespread use of cutting-edge technologies in the government and within the society, a series of monitoring and reporting mechanisms, complemented with information systems are in place which allow smart detection of hazardous events and infectious diseases. Significant improvements to these systems were put in place in recent years, following the Sewol Ferry disaster and the MERS-CoV outbreak, in order to increase information sharing between diverse platforms and to strengthen the infectious disease surveillance system.
As prescribed in the Act on the Management of Disasters and Safety, a whole-of-government system has been designed to monitor hazards, detect threats and define emergency levels. Linked to the Disaster Situation Information System (DSIS) managed by the MOIS National Disaster and Safety Control Center (NDSCC), the system gathers information from 15 ministries and agencies, ranging from the Korea Meteorological Agency for natural hazards, to the Korea Center for Disease Control for infectious diseases, which all have invested in robust monitoring and surveillance networks for the risks that they are in charge of (MOIS, 2018). Regarding healthcare information, the Emergency Medical Information Center (NEMC) also connects to the DSIS through its Disaster Emergency medical Service situation room established in 2014 (Cha et al., 2017[49]).
This state-of-the-art multi-hazard early warning systems enables timely detection for all the different types of emergencies which can endanger public health in Korea. The four-level categorisation of emergencies from attention (Blue), to caution (Yellow), alert (Orange) and serious (Red) with pre-defined thresholds, on which the system is based, (Table 4.6) is common for all hazards and threats. This approach facilitates a good understanding of risk levels across the large emergency response network and the society at large.
Redundant dissemination and two-ways communication make of the Korea warning system an advanced risk communication tool. Partnerships with telecommunication companies and broadcast media enables timely dissemination of warnings through a variety of channels. The Safemap application previously described is also used to provide direct warning to citizens, with a Cell Broadcasting System enabling warnings to reach citizens located in areas where safety is at threat and providing them with all the necessary information. Citizens can also report on disaster situations through the app back to the emergency responders, enabling crowdsourcing of risk information to get a clearer situation picture.
Regarding infectious diseases surveillance and detection, KCDC acts as the control tower of the National Notifiable Infectious Disease Surveillance System (NNIDSS), which is a robust country-wide system, to which all the medical institutions and personnel contribute. As per the Infectious Disease Control and Prevention Act, reporting is mandatory for 80 types of infectious diseases by all public and private healthcare facilities and laboratories, as well as for local governments. Medical personnel are to report 56 types of infectious diseases from Category 1 to Category 4 immediately through the dedicated information system. Category 3 influenza and Category 4 infectious diseases, and nationally identified infectious diseases, are reported through the sentinel surveillance system within seven days. NNIDSS builds on a solid network of 298 hospitals, 256 Public Health Centers, 13 quarantine stations and 17 Research Institute on Health and Environment with complementary national BSL-3 ad BSL-4 lab capacities (World Health Organisation, 2017[43]). In addition, for bio threats, a syndromic surveillance system is in place in all 132 emergency medical facilities of Korea to monitor and report suspected patients with acute rashes, haemorrhage, nervous, and respiratory symptoms.
While NNIDSS was designed according to best international standards (Park and Cho, 2014[50]), the 2015 MERS-CoV outbreak demonstrated weaknesses in the detection of the outbreak and communication to the population (Jung et al., 2019[51]). This led the government to strengthen the event-based surveillance system, to create a new Emergency Operation Center at KCDC, and to increase the reporting requirements for healthcare facilities. These improvements will certainly contribute to an improved capability to detect infectious diseases in Korea, but attention should be paid to the risk of reporting fatigue in health institutions over the years, in a system which might appear excessively burdensome.
4.4.2. Korea is currently investing in strengthening health infrastructures dedicated to emergencies to increase preparedness and safety following a series of failures
Similarly, Korea is investing significantly in strengthening its health infrastructure to cope more effectively with both infectious diseases and multi-casualty disasters. As health emergencies in the last years demonstrated preoccupying gaps in infectious disease control in hospitals, rapid availability of healthcare in large accidents, as well as safety concerns in health institutions (Cha et al., 2017[49]), these on-going investments and the strengthening of the regulatory framework appear particularly relevant to bridge these gaps. Nevertheless, sustaining these improvements overtime would require for Korea to properly resource operation and maintenance for these infrastructure, and maintain the momentum on safety improvements in hospitals with an equilibrated partnership with the private sector.
Following the MERS outbreak, MOHW conducted a detailed assessment of the infectious diseases control capacities over Korea in 2015, with the aim of responding to the identified weaknesses during the epidemic and investing in new capabilities across the healthcare system. This risk-based capability assessment was based on a series of criteria, including the distribution of health and medical resources, the living environment and the population, the frequency of infectious diseases and the proximity to airports and sea ports. As a result, MOHW set up an ambitious plan to raise the level of preparedness of health infrastructure throughout the country with a series of new capabilities (Box 4.6). While these investments are largely financed by KCDC, there is a need to ensure sufficient budget for the maintenance of these capabilities overtime (World Health Organisation, 2017[43]).
The large spread of the MERS-CoV in 2015 was mostly nosocomial and required to upgrade the capabilities of infectious disease hospitals in Korea. Following the MOHW risk-based capability assessment, 10 new hospitals were designated as infectious diseases hospitals, and are progressively equipped with an additional 198 negative pressure beds and isolated outpatients room. With these new capabilities, Korea has now 29 infectious diseases hospitals across its 16 main cities and provinces. In addition, 100 negative pressure beds will be installed per regulation across the central hospitals of Korea (i.e. in hospitals with more than 500 beds). Finally, MOHW plans to establish a central hospital to deal with infectious diseases in 2022, which would act as a control tower overseeing infectious diseases hospitals.
Source: Compiled by the Authors based on interviews conducted with health professionals in Korea and Ministry of Health and Welfare response to the questionnaire to inform the OECD Reviews of Public Health: Korea.
Regarding other public health risks, Korea has also designated disaster-base hospitals across its territory and expanded its number from 20 to 40 in 2015 with the revision of the Framework Act on the Management of Disaster and Safety (Cha et al., 2017[49]). These disaster-base hospitals constitute the backbone of the National Emergency Medical Center (NEMC) disaster response system: they host the local disaster Medical Assistance Teams (DMAT) which can be deployed on disaster scenes to provide healthcare. The increase of disaster base hospitals enables a better coverage of the national territory and population and improves medical response preparedness for disasters.
Finally, hospital safety is a major concern in Korea. Beyond the MERS nosocomial infections, hospital accidents frequently occur, as shown in the recent fire of the Sejong hospital of Miryang during which 41 people died. As the OECD country with the highest number of hospital beds per inhabitants, ensuring safety levels of these healthcare providers is a key issue for public safety. Korea’s hospital evaluation programme was revised in 2015, to increase its focus on safety. However, this programme is mandatory only for general, public and specialised hospitals, and the participation rate is particularly low (World Health Organisation, 2015[52]).
4.4.3. Korea plans large stocks of medical countermeasures and emergency supplies for emergency response
Emergency capabilities also include stockpiling of medical countermeasures for disease outbreaks, as well stocking emergency relief supplies for disasters. Korea’s stockpiling policy for medical countermeasures follows international standards. Based on its risk assessment, this policy is supported by a robust legal base with the Infectious Disease Control and Prevention Act and the Pharmaceutical Affairs Act, and is updated regularly, every 3 years.
As in most OECD countries, the stockpiling policy in Korea was significantly upgraded after the 2009 H1N1 outbreak. A National Stockpile Plan was designed and guidelines developed for stockpiling and its management and distribution. Five national stockpile centres are strategically positioned throughout the country and local governments also contribute on the distribution plan. In 2012, Korea was storing 13 million doses of antiviral drugs (Tamiflu: 73% and Relenza: 27%), covering 26% of its population (Lee et al., 2013[53]). Personal protection equipment’s and other medical countermeasures for the 11 priority diseases identified by KCDC are also stored in the National Stockpile. Following the MERS outbreak, changes were introduced to adopt a more dynamic stockpiling approach with a system for real time stockpiling management currently under implementation as well as a 5 year National Strategic Stockpile.
Regarding vaccines, in addition to pre pandemic stockpile, Korea has the appropriate mechanisms to introduce new vaccines in vase of need through the Vaccine Management Council and Committee for the Safe Supply of National Essential Medicine (World Health Organisation, 2017[43]). Korea has also a national stockpile of smallpox vaccine covering 80% of the population.
Beyond the health sector, each sector is also responsible for maintaining stockpiles for responses to emergencies under the Framework Act on the Management of Disasters and Safety. A joint resource utilisation system was initiated in 2014 to coordinate inventory management and material deployment across sectors and is currently in the process of implementation (World Health Organisation, 2017[43]).
4.4.4. Workforce development for public health emergency preparedness is an on-going priority in Korea
As for the other capabilities described in this chapter section, workforce development is amongst Korea’s priorities to strengthen its public health emergency preparedness. The Disaster Medical Assistance Teams were reformed and reinforced, MOHW is establishing a system of psychological support practitioners for disasters, and most significantly infectious diseases specialists are being hired and trained to reinforce KCDC and Public Health Centers throughout Korea. The challenge now is to make sure that these strategic investments in skills best contribute to strengthening the entire public health system where the most important needs are.
The slow response during the MERS outbreak convinced Korean decision-makers of the need to reinforce skills and staff in KCDC and across national and local governments for infectious diseases preparedness and control. After a recruitment campaign, KCDC now counts approximately 1 400 staff for prevention, investigation, quarantine, testing, and research of infectious diseases. The 10 KCDC’s Rapid Response Teams (RRT) can be deployed rapidly for epidemic investigations. For surge capacities during large-scale epidemics, complementary Emergency Investigation Officers are trained through the Field Epidemiology Training Program and private sector healthcare professionals can also be mobilised. In addition, MOIS is currently recruiting a total of 366 people in charge of infectious diseases at the subnational in the Public Health Centers (World Health Organisation, 2017[43]). At the local level, Public Health Centers and local governments are attentive to how these new resources will be distributed across the country as some fears it might not be risk-based.
For other public health emergencies, Korea also has adjusted its workforce. Disaster Medical Assistance Teams (DMAT) are now better able to rapidly deploy on disaster scenes and maintain a longer presence. Based on foreign experience, such as the Japan DMAT, these emergency healthcare providers’ teams have been reduced in size, dispatched in a larger number of disaster base hospitals throughout the country, reorganised and trained (Cha et al., 2017[49]). Furthermore, Korea MOHW aims also to develop dedicated process for the mobilisation of Disaster Psychological Assistance Teams (DPAT) to provide psychological support during and after disasters to affected populations. The National Center for Mental Health has initiated these reflexions in the aftermath of the Ferry Sewol Accident, which largely traumatised the Korean society (Jo et al., 2018[54]).
copy the linklink copied!4.5. Emergency countermeasures and their implementation during crisis
Korea has developed a set of emergency plans to mobilise its capabilities and implement countermeasures when public health crises occur. A large planning effort across levels of government and sectors based on the development of standard operating procedures contributes to improve preparedness, but this tends to favour silo-ed and rigid approaches. However, as shown in recent crises, inter-agency coordination grounded on regular multi-stakeholder exercises would need to be strengthened for a more flexible and adaptable crisis response in Korea, with improved crisis leadership and crisis communication.
As proposed by the OECD Recommendation on the Governance of Critical Risks, preparing better for the more complex and unforeseeable crises of today’s risk landscape requires going beyond standard operating procedures based on the history of past events to embrace agile multi-stakeholder partnerships. An encouraging dynamic is shaping up in this direction in Korea, which demonstrated a change of mind-set, but this remains an unfinished agenda.
4.5.1. Public health emergency plans are developed at all levels in Korea but this approach does not favour agile emergency response
In Korea, based on the overarching Master Plan for National Safety Management developed by MOIS, all ministries and agencies have to prepare a Standard Manual for Crisis Management for the emergencies they are responsible for. These 33 manuals cover all the national emergencies identified in the risk assessment and include 13 crisis management functions such as management, communication, financing, medical services, search and rescue, etc. (Jang and Yun, 2017[55]). Similarly, local plans are developed based on national guidelines by local governments.
Regarding public health specifically, MOHW is responsible for developing and maintaining the Standard Manual for Infectious Diseases Emergency Management as well as for supporting the function of supporting medical and disinfection services for other types of crises. KCDC, as the main operating agency for infectious diseases response has also developed a dedicated Operational Manual, detailing the standard operating procedures for engaging disease control countermeasures. Based on lessons learned during the MERS-CoV outbreak, these manuals are currently being updated.
This extensive development of emergency plans across Korea’s institutions and levels of governments has benefits, as it reinforces engagement, accountability and responsibility of stakeholders. Through yearly inspections of the plans from sectoral ministries to local governments, MOIS ensures that guidelines are followed. Furthermore, MOIS has set up incentives for local governments to develop qualitative plans: based on a series of indicators, rewards for high-quality preparedness and special grants to support strengthening for the ones showing weaknesses are allocated. A similar model exists in MOHW for the public health plans of local government, which also addresses public health emergency preparedness.
More efforts would nevertheless be required to ensure coherence between this large set of emergency plans. Based on the 33 types of crisis management manuals in Korea, departments created 278 crisis response manuals, 1 300 related organisations, and 2 339 on-site action manuals (Bang and Kim, 2016[56]). The multiplicity of plans makes it difficult to ensure coherence when a crisis strikes. As these manuals tend to favour a command and control system with pre-determined standard operating procedures (SOP), they have often generated silo-ed approaches and did not demonstrate sufficient flexibility when facing complex emergencies. While SOP are necessary for classic emergencies, more and more, OECD countries are adopting a multi-hazard approach based on flexible partnerships, robust leadership and regular exercises across a multi-stakeholder response network to prepare better for complex and unprecedented types of crises (OECD, 2018[1]).
4.5.2. Korea is making efforts to foster inter-agency coordination in public health emergency response
Evidence of coordination failures in crisis management have prompted a major reflection in Korea on inter agency coordination and crisis leadership. Both during the Ferry Sewol disaster and the MERS outbreak (Box 4.7), applying crisis manuals by individual organisations proved largely insufficient to reduce the public health consequences of these crises: crisis sense-making was affected by the absence of pan-governmental communication and information exchange, ineffective coordination between organisations led to delayed responses, lack of leadership made decision-making unclear.
The MERS epidemic outbreak demonstrated the importance of clarifying governance for crisis management in Korea. Both crisis coordination mechanisms and crisis leadership changed not less than four times during the outbreak, which led to major confusions in the response, and contributed to creating panic and deteriorating trust in government.
While KCDC established its Countermeasure Headquarter after the first patient was confirmed to be infected by MERS on May 20, 2015, MOHW took over the crisis control through its Central MERS management headquarters a few days after, as the infection was mostly nosocomial. Then, the Ministry of Public Safety and Security – now MOIS – set-up the Pan Government MERS Countermeasure Support Centre to ensure coordination across ministries and with local governments.
Source: Park, M. (2017[42]), “Infectious disease-related laws: prevention and control measures”, Epidemiology and Health, Vol. 39, p. e2017033, https://doi.org/10.4178/epih.e2017033.
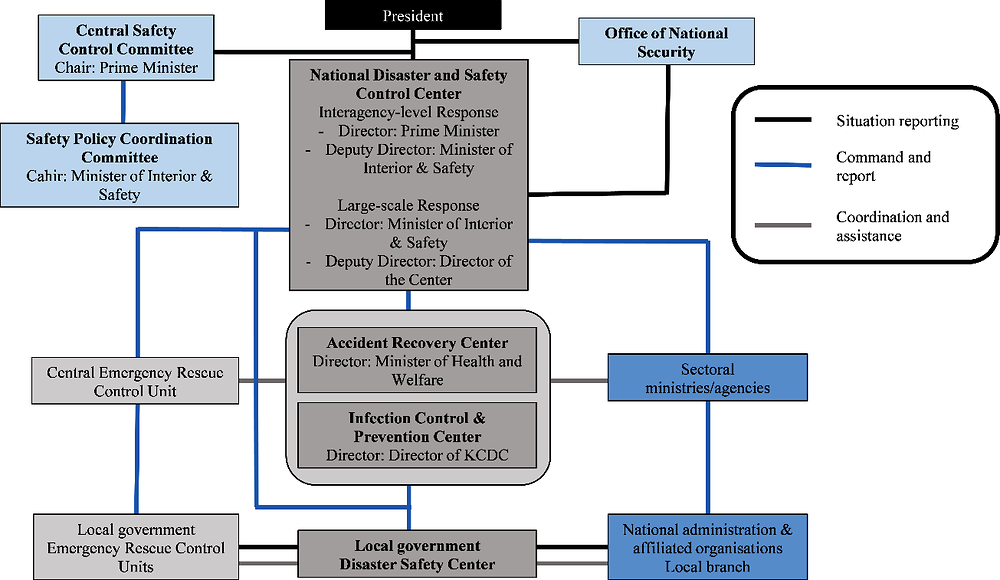
Since then, revisions to the governance of crisis management represent substantive changes towards improved interagency coordination. The establishment of the National Disaster Safety Control Center (NDSCC) under MOIS in 2015 as a joint situation center with representatives from all the relevant ministries and agencies is promising. The Centre is equipped with appropriate situation awareness and information sharing tools. A problem-solving doctrine has been core to its design, based on comprehensive situation judgement meetings. A direct link to political leadership facilitates decision-making, with the involvement of the Minister of the Interior and Safety or the Prime Minister, depending on the crisis’ scale (Figure 4.6).
Source: Compiled by the author based on responses of the Korea Authorities to the OECD questionnaire to inform the OECD Reviews of Public Health: Korea.
In the case of infectious diseases, KCDC has also strengthened its capacities to operate as an effective command and control center with its Emergency Operations Centre established in 2015. The Centre which operates on a 24/7 basis can operate as the Central Epidemic Control Countermeasure Headquarters if an infectious disease crisis is detected, under the leadership of the KCDC director or the Ministry of Health in case of severe crisis.
This new organisation clarifies leadership and facilitates inter-agency coordination. However the establishment of two new structures, NDSCC and KCDC EOC, requires specific arrangements to clarify their coordination mechanisms in case of a large-scale infectious disease outbreak. MOIS and the Prime Minister remain overarching coordinators during large scale events, and are also essential for ensuring a good coordination with local governments.
4.5.3. Revisiting approaches to crisis communication in Korea is a priority
Crisis communication is an essential part of emergency response. It is fundamental to convey critical messages for the safety and security of the population as well as to reduce citizens’ uncertainty during crises (OECD, 2015[44]). Good or poor crisis communication can significantly change the course of a crisis, both in terms of public health consequences (e.g. if citizens are not well informed of the countermeasures taken or that they should follow) and/or in terms of trust in government and public institutions (e.g. if the perception that the crisis is not well managed prevails).
During the MERS outbreak, public risk communication was delayed and resulted in a widespread panic. The government’s non-disclosure decision on the names of the hospitals where the infection had spread, significantly affected trust in government and in the health system (Kim et al., 2017[17]). One can understand the difficulty of crisis communication in light of the important uncertainties on the crisis’ status, future developments, and on the ways to handle it. Nevertheless, attention to citizens’ expectations and disarray is also fundamental to consider in crisis communication. Otherwise, there are risks that inadequate communication contributes to aggravating the crisis, as was the case during the MERS outbreak, and also during the Ferry Sewol disaster.
Korea invested in recent years to improve its crisis communication approach towards more transparency. KCDC for instance has established a dedicated Office of Communications in 2015, and mobilised the right skills by hiring communication professionals and media specialists, including to work on public perceptions. This resulted in the diffusion of crisis communication guidelines and SOPs for officials (KCDC, 2017[57]). In addition to using a variety of communication channels from media briefing, to web based platforms, social media, and call centres, there is a mechanism in place to promptly identify and manage rumours and misinformation through social networks (World Health Organisation, 2017[43]).
4.5.4. Multi-stakeholder emergency simulation exercises based on complex scenarios could be undertaken regularly
In Korea, simple exercises are undertaken regularly to test emergency plans and procedures, but simulation exercises based on more complex scenario including multiple stakeholders are necessary to improve its preparedness.
Every year, MOIS organises a national exercise with all the departments at the occasion of the Disaster Safe Korea day in May. Monthly exercises are also conducted for 22 types of crises, with scenarios, such as traffic accident, earthquakes, large fires, chemical accidents, bioterrorism or explosion of a nuclear reactor. On public health emergencies specifically, MOHW and KCDC also organise regular national exercises and simulation drills and has increased the number of these from 20 to 30, including a yearly large-scale drill. For instance in 2018, they organised a table-top exercise with 100 Public Health Centers. Smaller-scale drills at the local level are conducted every two years in each Public Health Centre.
All these exercises and drills are useful to ensure that procedures are well-known and tested, but most of them are based on testing the manuals and this approach may not be sufficient to prepare for complex emergencies. Indeed, these exercises often lack elements of surprise and complexity which would force crisis managers and officials to go out of their comfort zone as real emergencies require, and to detect areas of improvement. Beyond the yearly multi-stakeholder exercise on the Disaster Safe Korea day, such complex exercises should involve the entire network of emergency responders from the different sectoral ministries as well as the levels of government, the private sector and civil society. As more and more OECD countries are now utilising exercises to go beyond the testing of emergency procedures to learn lessons, identify deficiencies and improve policies and procedures, Korea could learn from these advanced approaches (OECD, 2018[1]).
copy the linklink copied!Conclusion
Korea has invested significantly in the last few years in restructuring and reinforcing its public health emergency preparedness policies and capabilities, notably following the Sewol Ferry Disaster in 2014, and the MERS-CoV epidemic outbreak in 2015. Both crises revealed major shortcomings in applying safety regulations, their control, and crisis management. This led to revisiting the legal framework, including the Framework Act on the Management and Disasters and Safety, and the Infectious Diseases Control and Prevention Act. There is now an all-hazards and threats approach to risk management although not yet a National Risk Assessment process in place that would allow to prioritise efforts across the different risks to public health in the country.
The institutional framework has been revised under the new Ministry of Interior and Safety, following a series of reforms. Regarding infectious diseases, the aftermath of the MERS epidemic led to a major strengthening of the Korea Center for Diseases Control, which revised its risk assessment and risk communication processes significantly. Investments in public health emergency capabilities across the board, from detection and information systems, to stockpiling of countermeasures and public health emergency workforce leave the overall system at the right level of capabilities in light of the Korean risk landscape. Korea is also making the best of innovation and technologies to foster timely detection, enable information-sharing from authorities to citizens, and facilitate decision-making.
Despite the usefulness of these necessary policy reforms and new capabilities, strengthening emergency preparedness in Korea remains an unfinished agenda. Overall, Korea appears to be over-reliant on planning at all the levels of its administration, which is important but not sufficient for preparedness for more complex and unforeseen emergencies. Strengthening capacities for a more agile response based on multi-stakeholder partnerships, flexible arrangements, and engaged leadership should be the guiding objectives for Korea to further progress in emergency preparedness. Furthermore, strengthening preparedness at the local level is a major priority. More work also needs to be done to address the main weakness of Korea’s public health system when it comes to infectious diseases prevention: because of the weak primary care system in Korea, Koreans rush to large hospitals for any symptom, which can contribute to spreading infections. Finally, it is also important to maintain the momentum to continue strengthening public health emergency preparedness capacities overtime, and prevent a fading-off of efforts, even in the absence of major crises. There is no place for complacency in emergency preparedness.
References
[32] Aldrich, N. and W. Benson (2008), “Disaster preparedness and the chronic disease needs of vulnerable older adults”, Preventing Chronic Disease, Vol. 5/1, http://www.cdc.gov/pcd/issues/2008/jan/07_0135.htm.
[6] Asia Sentinel (2012), “Seoul’s Lessons for Asian Urban Flooding”, https://www.asiasentinel.com/society/seouls-lessons-for-asian-urban-flooding/ (accessed on 22 January 2020).
[39] Bae, Y., Y. Joo and S. Won (2016), “Decentralization and collaborative disaster governance: Evidence from South Korea”, Habitat International, Vol. 52, pp. 50-56, https://doi.org/10.1016/j.habitatint.2015.08.027.
[28] Bae, Y., Y. Joo and S. Won (2015), “Decentralization and collaborative disaster governance Decentralization and collaborative disaster governance Decentralization and collaborative disaster governance: Evidence from South Korea”, https://doi.org/10.1016/j.habitatint.2015.08.027.
[56] Bang, M. and Y. Kim (2016), “Collaborative governance difficulty and policy implication”, Disaster Prevention and Management: An International Journal, Vol. 25/2, pp. 212-226, https://doi.org/10.1108/DPM-12-2015-0295.
[49] Cha, M. et al. (2017), “Changes to the Korean Disaster Medical Assistance System After Numerous Multi-casualty Incidents in 2014 and 2015”, Disaster Medicine and Public Health Preparedness, Vol. 11/05, pp. 526-530, https://doi.org/10.1017/dmp.2016.202.
[18] Cho, S. et al. (2016), “MERS-CoV outbreak following a single patient exposure in an emergency room in South Korea: an epidemiological outbreak study”, The Lancet, Vol. 388/10048, pp. 994-1001, https://doi.org/10.1016/S0140-6736(16)30623-7.
[29] Dostal, J., H. Kim and A. Ringstad (2015), A Historical-Institutionalist Analysis of the MV Sewol and MS Estonia Tragedies: Policy Lessons from Sweden for South Korea*, http://s-space.snu.ac.kr/bitstream/10371/94529/1/02_Jorg%20Michael%20Dostal.pdf (accessed on 11 February 2019).
[4] EM-DAT (2017), The International Disasters Database, https://www.emdat.be/ (accessed on 30 January 2020).
[26] Go, U. et al. (2018), Tuberculosis prevention and care in Korea: Evolution of policy and practice, Elsevier Ltd, https://doi.org/10.1016/j.jctube.2018.04.006.
[40] Government of Korea (2015), Framework Act on the Management of Disasters and Safety.
[47] Government of Korea (2015), Korea Infectious Diseases Prevention and Control Act.
[41] Heo, B., J. Park and W. Heo (2018), “Sustainable Disaster and Safety Management of Government: Integrated Disaster and Safety Budget System in Korea”, Sustainability, Vol. 10/11, p. 4267, https://doi.org/10.3390/su10114267.
[15] Hijioka, Y., E. Lin and J. Jacqueline Pereira (2014), Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B: Regional Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change, IPCC, Cambridge, https://www.ipcc.ch/site/assets/uploads/2018/02/WGIIAR5-Chap24_FINAL.pdf (accessed on 11 February 2019).
[24] Hong, S. and A. Collins (2006), “Societal Responses to Familiar Versus Unfamiliar Risk: Comparisons of Influenza and SARS in Korea”, Risk Analysis, Vol. 26/5, pp. 1247-1257, https://doi.org/10.1111/j.1539-6924.2006.00812.x.
[55] Jang, Y. and H. Yun (2017), Improving Disaster Management System in Korea for Effective Disaster Response, https://doi.org/10.17758/EIRAI.H0217308.
[12] Jeong, D. (2008), “Socio-Economic Costs from Yellow Dust Damages in South Korea”, Korean Social Science Journal, Vol. XXXV/No.2, pp. 1-29.
[54] Jo, S. et al. (2018), “Decision Making Regarding Key Elements of Korean Disaster Psychiatric Assistance Teams Using the Analytic Hierarchy Process”, Psychiatry Investigation, Vol. 15/7, pp. 663-669, https://doi.org/10.30773/pi.2018.01.13.
[51] Jung, J. et al. (2019), “Complementing conventional infectious disease surveillance with national health insurance claims data in the Republic of Korea”, Scientific Reports, Vol. 9/1, https://doi.org/10.1038/s41598-019-45409-3.
[45] Kang, H. (2016), Disaster Early Warning Services in the Republic of Korea, http://www.safekorea.go.kr/ids (accessed on 11 February 2019).
[27] KCDC (2018), National TB Elimination Project, http://www.cdc.go.kr/contents.es?mid=a30301120000 (accessed on 22 January 2020).
[57] KCDC (2017), Standard Operating Procedure for Risk Communication for Public health Emergencies, http://www.cdc.go.kr/CDC/cms/cmsFileDownload.jsp?fid=51&cid=138103&fieldName=attach1&index=1 (accessed on 15 January 2019).
[16] Ki, M. (2015), “2015 MERS outbreak in Korea: hospital-to-hospital transmission.”, Epidemiology and health, Vol. 37, p. e2015033, https://doi.org/10.4178/epih/e2015033.
[14] Kim, D. (2017), “Mapping heatwave vulnerability in Korea”, Natural Hazards - Journal of the International Society for the Prevention and Mitigation of Natural Hazards, https://doi.org/10.1007/s11069-017-2951-y.
[21] Kim, J. (2016), “The 2009 H1N1 Pandemic Influenza in Korea”, Tuberculosis and Respiratory Diseases, Vol. 79/2, p. 70, https://doi.org/10.4046/trd.2016.79.2.70.
[19] Kim, J. et al. (2010), “The Spread of Pandemic H1N1 2009 by Age and Region and the Comparison among Monitoring Tools”, Journal of Korean Medical Science, Vol. 25/7, p. 1109, https://doi.org/10.3346/jkms.2010.25.7.1109.
[17] Kim, K. et al. (2017), “Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in South Korea, 2015: epidemiology, characteristics and public health implications”, Journal of Hospital Infection, Vol. 95/2, pp. 207-213, https://doi.org/10.1016/J.JHIN.2016.10.008.
[22] Kim, Y., S. Yoon and I. Oh (2013), “The economic burden of the 2009 pandemic H1N1 influenza in Korea”, Scandinavian Journal of Infectious Diseases, Vol. 45/5, pp. 390-396, https://doi.org/10.3109/00365548.2012.749423.
[9] Korea Meteorological Administration (2018), Annual report 2017, https://web.kma.go.kr/download_01/Annual_Report_2017.pdf (accessed on 11 February 2019).
[8] Korea Meteorological Administration (2017), ANNUAL REPORT 2016, https://web.kma.go.kr/download_01/Annual_Report_2016.pdf (accessed on 11 February 2019).
[34] Korea Tourism Organisation (2019), Korea, Monthly Statistics of Tourism | key facts on toursim | Tourism Statistics, https://kto.visitkorea.or.kr/eng/tourismStatics/keyFacts/KoreaMonthlyStatistics.kto (accessed on 11 February 2019).
[53] Lee, H. et al. (2013), “Public Health Crisis Preparedness and Response in Korea”, Osong Public Health and Research Perspectives, Vol. 4/5, pp. 278-284, https://doi.org/10.1016/J.PHRP.2013.09.008.
[7] Lee, J. et al. (2018), “Seismicity of the 2016 M L 5.8 Gyeongju earthquake and aftershocks in South Korea”, Geosciences Journal, Vol. 22/3, pp. 433-444, https://doi.org/10.1007/s12303-017-0071-z.
[46] Ministry of the Interior and Safety (2019), Integrated Disaster and Safety Information System, https://www.mois.go.kr/eng/sub/a03/bestPractices1/screen.do (accessed on 30 January 2020).
[11] Na, W. et al. (2013), “The Effects of Temperature on Heat-related Illness According to the Characteristics of Patients During the Summer of 2012 in the Republic of Korea”, Journal of Preventive Medicine & Public Health, Vol. 46/1, pp. 19-27, https://doi.org/10.3961/jpmph.2013.46.1.19.
[35] OECD (2019), “Metropolitan areas”, OECD Regional Statistics (database), https://dx.doi.org/10.1787/data-00531-en (accessed on 22 January 2019).
[10] OECD (2019), OECD Reviews of Public Health: Japan: A Healthier Tomorrow, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264311602-en.
[1] OECD (2018), Assessing Global Progress in the Governance of Critical Risks, OECD Reviews of Risk Management Policies, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264309272-en.
[13] OECD (2018), National Risk Assessments: A Cross Country Perspective, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264287532-en.
[36] OECD (2018), OECD Health Statistics 2018 - OECD, http://www.oecd.org/health/health-data.htm (accessed on 11 February 2019).
[48] OECD (2018), OECD Toolkit on Risk Governance, https://www.oecd.org/governance/toolkit-on-risk-governance/home/ (accessed on 22 January 2020).
[30] OECD (2018), Working Better with Age: Korea, Ageing and Employment Policies, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264208261-en.
[44] OECD (2015), The Changing Face of Strategic Crisis Management, OECD Reviews of Risk Management Policies, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264249127-en.
[2] OECD/KDI (2018), Understanding the Drivers of Trust in Government Institutions in Korea, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264308992-en.
[38] Park, J. et al. (2010), “Perceptions and behaviors related to hand hygiene for the prevention of H1N1 influenza transmission among Korean university students during the peak pandemic period”, BMC Infectious Diseases, Vol. 10/1, p. 222, https://doi.org/10.1186/1471-2334-10-222.
[42] Park, M. (2017), “Infectious disease-related laws: prevention and control measures”, Epidemiology and Health, Vol. 39, p. e2017033, https://doi.org/10.4178/epih.e2017033.
[50] Park, S. and E. Cho (2014), “National Infectious Diseases Surveillance data of South Korea”, Epidemiology and Health, p. e2014030, https://doi.org/10.4178/epih/e2014030.
[3] Reuters (2015), “South Korea replaces health minister criticized over MERS outbreak - Reuters”, https://www.reuters.com/article/us-health-mers-southkorea-idUSKCN0Q90JJ20150804 (accessed on 22 January 2020).
[5] Reuters (2011), “UPDATE 2-S.Koreans on landmine alert after deadly mudslides - Reuters”, https://www.reuters.com/article/korea-weather/update-2-s-koreans-on-landmine-alert-after-deadly-mudslides-idUSL3E7IS0M620110728 (accessed on 22 January 2020).
[37] Ryu, S. (2017), “The new Korean action plan for containment of antimicrobial resistance”, Journal of Global Antimicrobial Resistance, Vol. 8, pp. 70-73, https://doi.org/10.1016/J.JGAR.2016.10.013.
[23] Takahashi, S. et al. (2017), “Public preventive awareness and preventive behaviors during a major influenza epidemic in Fukui, Japan”, Journal of Infection and Public Health, Vol. 10/5, pp. 637-643, https://doi.org/10.1016/J.JIPH.2017.04.002.
[31] UNEP (ed.) (2016), Global Assessment of Sand and Dust Storms, http://www.un.org/Depts/Cartographic/english/htmain.htm (accessed on 11 February 2019).
[25] World Health Organisation (2018), Tuberculosis country profiles, https://www.who.int/tb/country/data/profiles/en/ (accessed on 17 January 2019).
[43] World Health Organisation (2017), Joint External Evaluation of IHR Core CapacitiesREPUBLIC OF KOREA, https://apps.who.int/iris/bitstream/handle/10665/259943/WHO-WHE-CPI-2017.65-eng.pdf?sequence=1 (accessed on 11 February 2019).
[52] World Health Organisation (2015), Korea Health System Review Health Systems in Transition, https://apps.who.int/iris/bitstream/handle/10665/208215/9789290617105_eng.pdf?sequence=1&isAllowed=y (accessed on 11 February 2019).
[33] Yoo, M., M. Lee and D. Tullmann (2016), “Perceptions of disaster preparedness among older people in South Korea”, International Journal of Older People Nursing, Vol. 11/1, pp. 18-23, https://doi.org/10.1111/opn.12084.
[20] Yun, J. et al. (2017), “The Korean Influenza National Immunization Program: History and Present Status”, Infection & Chemotherapy, Vol. 49/4, p. 247, https://doi.org/10.3947/ic.2017.49.4.247.
Metadata, Legal and Rights
https://doi.org/10.1787/be2b7063-en
© OECD 2020
The use of this work, whether digital or print, is governed by the Terms and Conditions to be found at http://www.oecd.org/termsandconditions.
