
1. Why physical activity?
Regular physical activity has a wide range of health and well-being benefits. This chapter provides an overview of these benefits. It also outlines the frequency, intensity, type and duration of physical activity that is recommended for different population groups. Finally, it describes the current policy measures that are in place in the European Union to encourage physical activity in the population.
Regular physical activity is one of the most important things people can do to improve their physical and mental health and well-being, regardless of age, sex or ethnicity.
Insufficient physical activity is a leading risk factor for non-communicable diseases such as cardiovascular diseases, type 2 diabetes, cancers, and has a negative effect on mental health and quality of life.
A low amount of physical activity, a low level of fitness and sedentariness – although interlinked – all independently increase the risk of many chronic diseases.
In 2020, the World Health Organization launched new physical activity guidelines, which recommend that adults should do at least 150 to 300 minutes of moderate-intensity physical activity per week, or 75 to 150 minutes of vigorous intensity physical activity.
There are growing policy making efforts across the European Union aimed to increase population-level physical activity.
Regular physical activity is one of the most important things people can do to improve their physical and mental health and well-being. Moving more and sitting less have benefits for everyone, regardless of age, sex, race, ethnicity or current fitness level. Considering both the impact of the COVID-19 pandemic and the increasing burden of non-communicable diseases and mental health conditions, physical activity is now more important than ever.
Currently, the world is experiencing an extraordinary, life-altering challenge due to the COVID-19 pandemic. But while the pandemic is having devastating human and economic consequences, it should not make people lose sight of the impact of major risk factors on the burden of chronic diseases, which also bear an increasing toll on mortality. Comparing COVID-19 related deaths to other common causes of death during the first wave in seven of the most affected European countries shows that, while mortality from COVID-19 was high particularly in elderly people, it was outweighed by deaths from cancer as well as cardiovascular diseases in Italy, Germany, France, Portugal and the Netherlands (Olabi et al., 2021[1]). In Spain the proportion of deaths due to COVID-19 was similar to that due to cancer. Moreover, the COVID-19 mortality rate is now declining further as treatments improve and vaccination coverage increases.
Life expectancy now reaches 81 years in the European Union (EU) (OECD/European Union, 2020[2]; World Bank, 2019[3]). However, many years of life in old age are lived with chronic diseases and disabilities. The main cause of death is still non-communicable diseases (NCDs) across Europe. In the EU Member States cardiovascular diseases (over 1 700 000 deaths in 2017) and cancers (1 200 000 deaths) together account for over 60% of all deaths. Nearly 40% of people aged 65 years and over have at least two chronic conditions, although this does not necessarily impede them from leading a normal life. About 30% of people aged 65 years and over have at least one limitation in activities of daily living that may require some long-term care assistance (OECD/European Union, 2020[2]).
Good mental health is vital for people to be able to lead healthy and productive lives. In 2018, one in nine adults (11%) on average across EU Member States had symptoms of psychological distress (OECD/European Union, 2020[2]). Currently, the situation maybe even worse as the COVID-19 crisis is also having a negative impact on mental well-being, especially amongst young people and people with lower socio-economic status (Aknin et al., 2021[4]). Moreover, the population in the EU is older than the global population, suggesting that it might be particularly vulnerable to an increasing burden of age-related neurological disorders, such as stroke or Alzheimer disease, which ranked third after cardiovascular diseases and cancers – representing 13.3% of total disability adjusted life years (DALYs) and 19.5% of total deaths (Deuschl et al., 2020[5]).
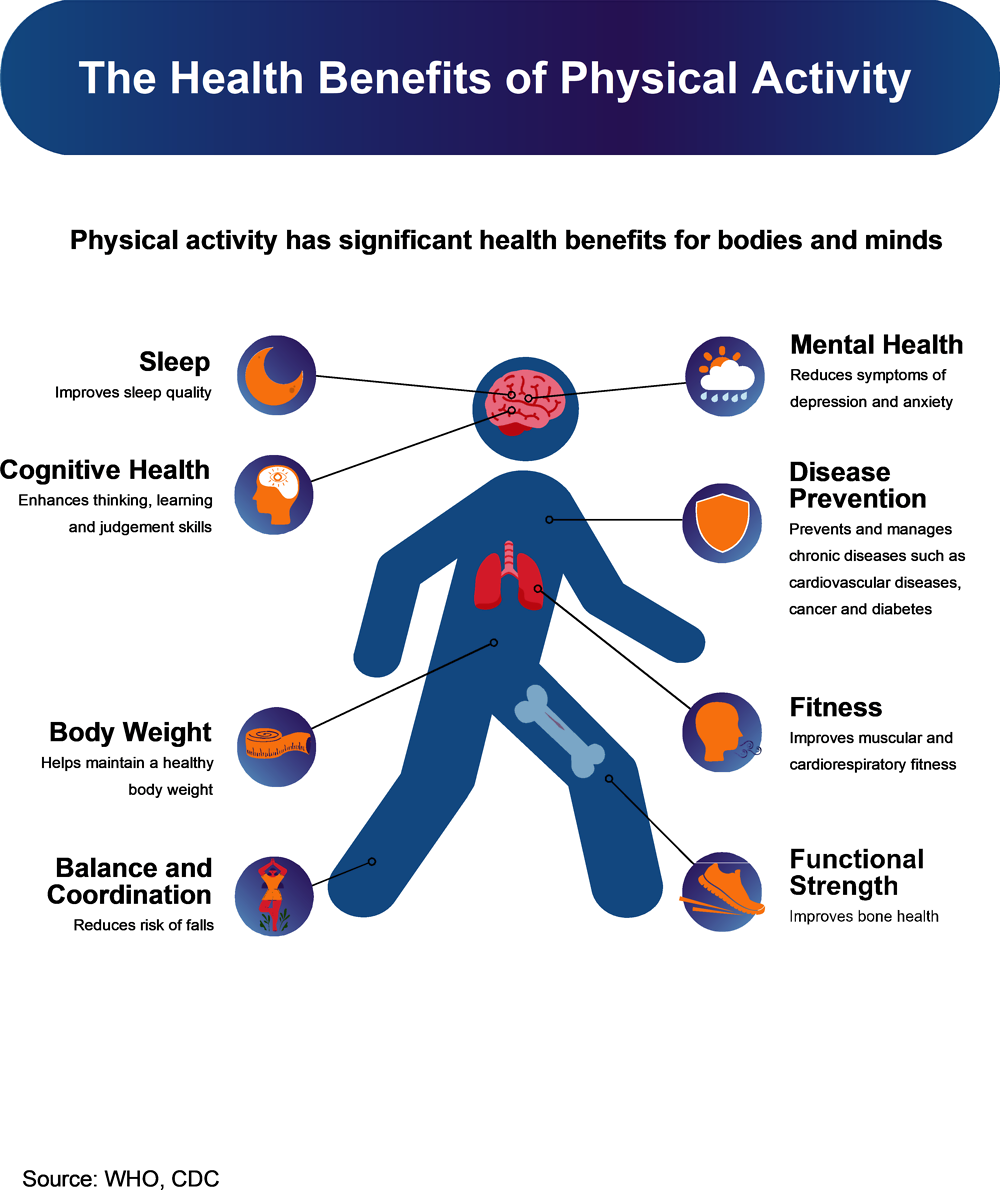
Fortunately, the majority of the most common chronic diseases and mental disorders are favourably influenced by regular physical activity. Even a single session of moderate-to-vigorous physical activity can reduce blood pressure, improve insulin sensitivity, improve sleep, reduce anxiety symptoms, and improve some aspects of cognition (including attention and memory) on the day that it is performed (Department of Health and Human Services, 2018[6]). Most of these improvements become even larger with the regular performance of physical activity. Other benefits, such as disease risk reduction and improved physical function, occur within days to weeks after consistently being more physically active.
Evidence shows that regular physical activity reduces all-cause mortality, as well as the risk of coronary heart disease, high blood pressure, stroke, insulin resistance, type 2 diabetes, some types of cancers, depression, anxiety, neuro-degenerative diseases and falls. Other benefits include increased cardiorespiratory and muscular fitness (Box 1.1), enhanced immune system, healthier body mass and composition, improved bone health, increased functional health, improved cognitive function and better sleep (Lee et al., 2012[7]).
There are three independent risk factors that are linked to someone’s activity habits and lifestyle. These are a low amount of physical activity, a low level of cardiovascular fitness (CVF) and sedentary behaviour. Although these factors are interlinked, they all independently increase the risk of chronic diseases.
Even if, at first, insufficient physical activity and sedentary behaviour sound very similar, they are conceptually different (van der Ploeg and Hillsdon, 2017[8]). Insufficient physical activity occurs when individuals are not meeting the requirements of current physical activity guidelines. In contrast, sedentary behaviour is any behaviour during waking hours characterised by a low energy expenditure while sitting, reclining or lying. Sedentary behaviour includes most desk-based office work, driving a car, TV-watching and playing inactive video games and it is often estimated by sitting time or screen time (WHO, 2020[9]; SBRN Terminology Consensus Project Participants, 2017[10]). Research on the health effects of sedentary behaviour is a relatively new area, but the potential population health impact of sedentariness is substantial (Biddle et al., 2016[11]).
CVF is a direct marker of physiologic status and reflects the overall capacity of the cardiovascular and respiratory systems, and the ability to carry out prolonged physical exercise. Recent data suggest that CVF has an important role in reducing not only cardiovascular and all-cause mortality, but also incident myocardial infarction, hypertension, diabetes, atrial fibrillation, heart failure, and stroke (Al-Mallah, Sakr and Al-Qunaibet, 2018[12]). Most recently, its role in cancer prevention has started to emerge. Moreover, high CVF during childhood and adolescence has been associated with a healthier cardiovascular profile during these years, as well as later in life (Ruiz et al., 2007[13]). The prognostic value of CVF has been demonstrated in various patient populations and in different cardiovascular conditions.
Physical inactivity, sedentary behaviour and low levels of fitness are all modifiable risk factors. Therefore, every individual should be encouraged to be physically active while limiting their time in sedentary activities to achieve optimal health benefits.
Physical activity is important for everyone at every stage of life. Just a few of the benefits for different population groups are (Department of Health and Human Services, 2018[6]):
Healthy growth and development, improved bone health and weight status for children ages 3 through 5 years.
Improved cognitive function, cardiorespiratory and muscle fitness, bone health and maintenance of healthy weight status for youth ages 6 to 13 years.
Brain health benefits, including possible improved cognitive function, reduced anxiety, depression and cognitive impairment risk, and improved sleep and quality of life across the lifespan.
For pregnant women, reduced risk of excessive weight gain, gestational diabetes, and postpartum depression.
For older adults, reduced risk of fall-related injuries, preserving physical function and mobility, and delaying the onset of major disability.
Current evidence suggests that many of the health benefits of a physically active lifestyle during adolescents carry forward into adulthood (Department of Health and Human Services, 2018[6]). Individuals who remain active throughout childhood and adolescence significantly reduce the risk of developing obesity in young adulthood (Kwon et al., 2015[14]). Physical activity also functions as a protective mechanism for depressive symptoms across all ages (Department of Health and Human Services, 2018[6]).
The positive health outcomes resulting from physical activity demonstrate that it is a “best buy” in the prevention and management of NCDs, improving daily functioning, mental health and well-being (van der Ploeg and Bull, 2020[15]). Europe’s demographic changes (ageing workforce and population) and the ongoing and after effects from the COVID-19 pandemic are highlighting the urgency for all countries in the WHO European Region to increase investment in policy, research and community-based programs to promote and ensure physical activity opportunities for everyone.
Physical activity goes beyond sports and exercise, and is defined as any bodily movement resulting in an increase in energy expenditure. Physical activity is evaluated by applying the FITT principles: F = frequency, I = intensity, T = time and T = type. Frequency denotes how often a person is physically active, intensity measures how vigorous the physical activity is; and time is the total duration of the activity. The type of physical activity refers to whether the activity is aerobic or anaerobic (e.g. cycling or sprinting), or can be categorised into three domains (i.e. leisure-time, transportation, work/household-related activities) (Rhodes et al., 2017[16]). Fundamentally, being physically active can be done in many ways: walking, cycling, sports and active forms of recreation (i.e. dance, yoga, swimming), activities at work, household and domestic duties. All forms of physical activity provide health benefits. However, when physical activity is practiced regularly, with sufficient duration and intensity, the benefits are greater (Rhodes et al., 2017[16]).
In 2020, WHO released new guidelines on physical activity and sedentary behaviour (Box 1.2). The guidelines recommend at least 150-300 minutes of moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity throughout the week for adults (including elderly, pregnant women and those with chronic medical conditions and/or disability all without contradictions) to achieve the above-mentioned benefits. For children and adolescents (5-17 years) the guidelines call for more activity.
To help reduce the detrimental effects of insufficient physical activity on health, all individuals are encouraged to become active. In addition to the physical activity recommendations below (Infographics 1.2 to 1.5), it is recommended for all individuals to limit the amount of time spent being sedentary. The guidelines also provide specific recommendations for individuals with chronic medical conditions and/or disability, and pregnant and postpartum women (see Annex 1.A for more detailed guidelines).
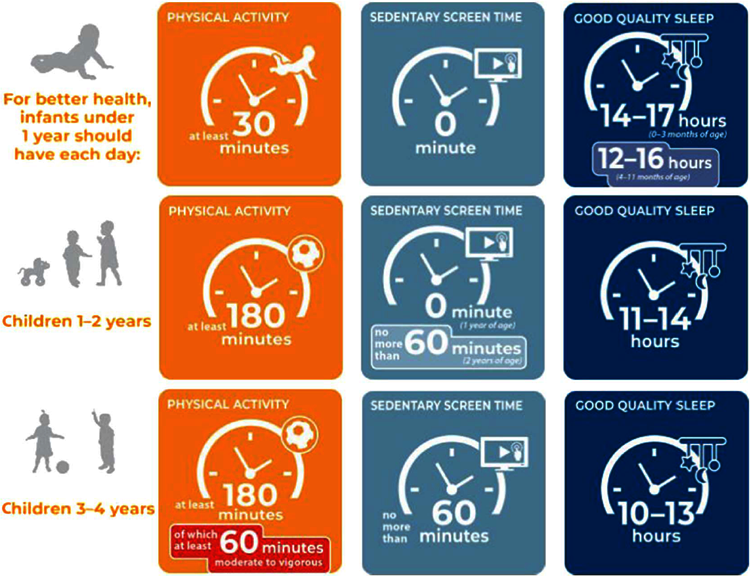



Source: WHO (2020[9]), WHO guidelines on physical activity and sedentary behaviour, https://www.who.int/publications/i/item/9789240015128; WHO (WHO, 2019[17]), Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age, https://apps.who.int/iris/bitstream/handle/10665/311664/9789241550536-eng.pdf?sequence=1&isAllowed=y
The majority of physical activity policy documents launched before 2010 dealt either with health-related behaviours in general or with nutrition and physical activity combined (Gelius et al., 2021[18]). Due to increasingly conclusive evidence regarding physical activity as a significant health determinant, there are growing policy making efforts aimed specifically to increase population-level physical activity, both at national and at international level.
In 2013, ministers of health and representatives of the Member States of WHO European Region adopted the Vienna Declaration on Nutrition and NCDs in the context of Health 2020. The declaration called for the development of an independent strategy to promote physical activity in the WHO European Region (WHO, 2013[19]). Since then WHO Europe and the European Commission have released regional strategies to promote and support policies to tackle physical inactivity and sedentary behaviours. Many members of the WHO European Region have established national physical activity policies in recent years to address the problem of physical inactivity (Figure 1.1). However, there remain challenges and opportunities to develop and improve the design and implementation of these policies, before the current physical inactivity trends and negative effects are reversed (WHO, 2021[20]).
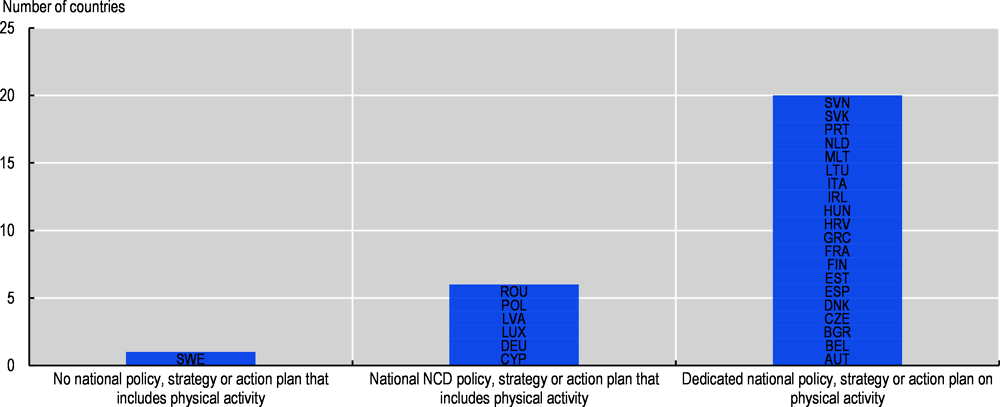
Source: WHO (2019[21]), NCD Country Capacity Survey, https://www.who.int/teams/ncds/surveillance/monitoring-capacity/ncdccs.
Also in 2013, Member States in the EU have adopted policies in line with the EU Council Recommendation on promoting health-enhancing physical activity (HEPA) across sectors (Council of the European Union, 2013[22]). The EU council recommendations include 23 indicators to measure progress on physical activity. The following year the Commission established a network of physical activity focal points to monitor the implementation of HEPA policies in the Member States, based on the EU Physical Activity Guidelines and the EU Council Recommendation (Whiting et al., 2021[23]). This was reinforced by the WHO Physical Activity Strategy for the WHO European Region 2016-25, which provided a blueprint to incentivise Member States to act (WHO, 2016[24]; Breda et al., 2018[25]). The European Commission in partnership with WHO Europe has published EU Member States factsheets on physical activity, which also provide an indication of the policy gaps that require more action at the national level (WHO, 2018[26]).
The WHO’s Global Action Plan on Physical Activity (GAPPA) 2018-30 was launched in 2018. The aim is to assist countries in developing policy actions to promote physical activity and to reduce physical inactivity by 10% by 2025, and 15% by 2030. This plan provides an evidence-based framework with four strategic objectives (active societies, active environment, active people and active systems) and 20 recommended policy actions and interventions (WHO, 2018[27]). Countries are encouraged to implement the GAPPA recommendations together with the ACTIVE technical package. This comprises a set of specific policy actions for governments at the national, sub-national and local level to promote physical activity throughout life and through multiple settings.
Finally, the two-year campaign HealthyLifestyle4All (HL4A) (EC, 2021[28]), which is a follow-up of the Tartu Call for a Healthy Lifestyle, was launched in September 2021 to showcase the European Commission’s continuous commitment to promoting a healthy lifestyle across generations and social groups.
References
[4] Aknin, L. et al. (2021), “Mental Health During the First Year of the COVID-19 Pandemic: A Review and Recommendations for Moving Forward”, In press at Perspectives on Psychological Science, https://doi.org/10.31234/OSF.IO/ZW93G.
[12] Al-Mallah, M., S. Sakr and A. Al-Qunaibet (2018), “Cardiorespiratory Fitness and Cardiovascular Disease Prevention: an Update”, Current Atherosclerosis Reports, Vol. 20/1, https://doi.org/10.1007/s11883-018-0711-4.
[11] Biddle, S. et al. (2016), “Too much sitting and all-cause mortality: is there a causal link?”, BMC Public Health, Vol. 16/1, https://doi.org/10.1186/s12889-016-3307-3.
[25] Breda, J. et al. (2018), “Promoting health-enhancing physical activity in Europe: Current state of surveillance, policy development and implementation”, Health Policy, Vol. 122/5, pp. 519-527, https://doi.org/10.1016/j.healthpol.2018.01.015.
[22] Council of the European Union (2013), “Council Recommendation of 26 November 2013 on promoting health-enhancing physical activity across sectors”.
[6] Department of Health and Human Services (2018), 2018 Physical Activity Guidelines Advisory Committee Scientific Report.
[5] Deuschl, G. et al. (2020), “The burden of neurological diseases in Europe: an analysis for the Global Burden of Disease Study 2017”, The Lancet Public Health, Vol. 5/10, pp. e551-e567, https://doi.org/10.1016/s2468-2667(20)30190-0.
[28] EC (2021), The HealthyLifestyle4All Initiative, https://sport.ec.europa.eu/initiatives/healthylifestyle4all (accessed on 20 October 2021).
[18] Gelius, P. et al. (2021), “Policy Instruments for Health Promotion: A Comparison of WHO Policy Guidance for Tobacco, Alcohol, Nutrition and Physical Activity”, International Journal of Health Policy and Management, https://doi.org/10.34172/ijhpm.2021.95.
[14] Kwon, S. et al. (2015), “Active lifestyle in childhood and adolescence prevents obesity development in young adulthood”, Obesity, Vol. 23/12, pp. 2462-2469, https://doi.org/10.1002/oby.21262.
[7] Lee, I. et al. (2012), “Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy”, The Lancet, Vol. 380/9838, pp. 219-229, https://doi.org/10.1016/s0140-6736(12)61031-9.
[2] OECD/European Union (2020), Health at a Glance: Europe 2020: State of Health in the EU Cycle, OECD Publishing, Paris, https://doi.org/10.1787/82129230-en.
[1] Olabi, B. et al. (2021), “Population perspective comparing COVID-19 to all and common causes of death during the first wave of the pandemic in seven European countries”, Public Health in Practice, Vol. 2, p. 100077, https://doi.org/10.1016/j.puhip.2021.100077.
[16] Rhodes, R. et al. (2017), “Physical activity: Health impact, prevalence, correlates and interventions”, Psychology & Health, Vol. 32/8, pp. 942-975, https://doi.org/10.1080/08870446.2017.1325486.
[13] Ruiz, J. et al. (2007), “High Cardiovascular Fitness Is Associated with Low Metabolic Risk Score in Children: The European Youth Heart Study”, Pediatric Research, Vol. 61/3, pp. 350-355, https://doi.org/10.1203/pdr.0b013e318030d1bd.
[10] SBRN Terminology Consensus Project Participants (2017), “Sedentary Behavior Research Network (SBRN) – Terminology Consensus Project process and outcome”, International Journal of Behavioral Nutrition and Physical Activity, Vol. 14/1, https://doi.org/10.1186/s12966-017-0525-8.
[15] van der Ploeg, H. and F. Bull (2020), “Invest in physical activity to protect and promote health: the 2020 WHO guidelines on physical activity and sedentary behaviour”, International Journal of Behavioral Nutrition and Physical Activity 2020 17:1, Vol. 17/1, pp. 1-4, https://doi.org/10.1186/S12966-020-01051-1.
[8] van der Ploeg, H. and M. Hillsdon (2017), “Is sedentary behaviour just physical inactivity by another name?”, International Journal of Behavioral Nutrition and Physical Activity, Vol. 14/1, https://doi.org/10.1186/s12966-017-0601-0.
[23] Whiting, S. et al. (2021), “Promoting health-enhancing physical activity in Europe: Surveillance, policy development and implementation 2015–2018”, Health Policy, Vol. 125/8, pp. 1023-1030, https://doi.org/10.1016/j.healthpol.2021.05.011.
[20] WHO (2021), 2021 physical activity factsheets for the European Union Member States in the WHO European Region, World Health Organization Regional Office for Europe, https://apps.who.int/iris/handle/10665/345335.
[9] WHO (2020), WHO guidelines on physical activity and sedentary behaviour, World Health Organization, https://apps.who.int/iris/handle/10665/336656.
[17] WHO (2019), Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age, World Health Organization, https://apps.who.int/iris/handle/10665/311664.
[21] WHO (2019), NCD Country Capacity Survey, https://www.who.int/teams/ncds/surveillance/monitoring-capacity/ncdccs (accessed on 27 October 2021).
[26] WHO (2018), European Health Information Gateway - Health-enhancing physical activity, https://gateway.euro.who.int/en/datasets/hepa/ (accessed on 20 October 2021).
[27] WHO (2018), Global action plan on physical activity 2018-2030, World Health Organization, https://apps.who.int/iris/handle/10665/272722.
[24] WHO (2016), Physical activity strategy for the WHO European Region 2016–2025, World Health Organization Regional Office for Europe, https://apps.who.int/iris/handle/10665/329407.
[19] WHO (2013), Vienna Declaration on Nutrition and Noncommunicable Diseases in the Context of Health 2020, World Health Organization Regional Office for Europe, https://apps.who.int/iris/handle/10665/350439.
[3] World Bank (2019), Life expectancy at birth, total (years), https://data.worldbank.org/indicator/SP.DYN.LE00.IN (accessed on 20 October 2021).
Infants under 1 year of age should be physically active several times a day in a variety of ways, particularly through interactive floor-based play; more is better. For those not yet mobile, this includes at least 30 minutes in prone position (tummy time) spread throughout the day while awake. They should not be restrained for more than 1 hour at a time (e.g. prams/ strollers, high chairs, or strapped on a caregiver’s back). Screen time is not recommended. When sedentary, engaging in reading and storytelling with a caregiver is encouraged. They should have 14-17 hours (0-3 months of age) or 12-16 hours (4-11 months of age) of good quality sleep, including naps (WHO, 2019[17]).
Children 1 and 2 years of age should spend at least 180 minutes in a variety of types of physical activities at any intensity, including moderate to vigorous-intensity physical activity, spread throughout the day; more is better. They should not be restrained for more than 1 hour at a time (e.g. prams/ strollers) or sit for extended periods of time. Sedentary screen time should be no more than 1 hour a day; less is better. When sedentary, engaging in reading and storytelling with a caregiver is encouraged. For 1-year-olds, sedentary screen time (such as watching TV or videos, playing computer games) is not recommended. For those aged 2 years, sedentary screen time should be no more than 1 hour a day; less is better. When sedentary, engaging in reading and storytelling with a caregiver is encouraged. They should have 11-14 hours of good quality sleep, including naps, with regular sleep and wake-up times (WHO, 2019[17]).
Children 3 and 4 years of age should spend at least 180 minutes in a variety of types of physical activities at any intensity, of which at least 60 minutes is moderate- to vigorous intensity physical activity, spread throughout the day; more is better. They should not be restrained for more than 1 hour at a time (e.g. prams/ strollers) or sit for extended periods of time. Sedentary screen time should be no more than 1 hour a day; less is better. When sedentary, engaging in reading and storytelling with a caregiver is encouraged. They should have 10-13 hours of good quality sleep, which may include a nap, with regular sleep and wake-up times (WHO, 2019[17]).
Children and adolescents should do at least an average of 60 minutes per day of moderate- to vigorous-intensity, mostly aerobic, physical activity, across the week. Vigorous-intensity aerobic activities, as well as those that strengthen muscle and bone, should be incorporated at least 3 days a week. Children and adolescents should limit the amount of time spent being sedentary, particularly the amount of recreational screen time (WHO, 2020[9]).
All adults should undertake regular physical activity. Adults should do at least 150-300 minutes of moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity throughout the week, for substantial health benefits. Adults should also do muscle strengthening activities at moderate or greater intensity that involve all major muscle groups on 2 or more days a week, as these provide additional health benefits. Adults should limit the amount of time spent being sedentary. Replacing sedentary time with physical activity of any intensity (including light intensity) provides health benefits. To help reduce the detrimental effects of high levels of sedentary behaviour on health, adults should aim to do more than the recommended levels of moderate- to vigorous-intensity physical activity (WHO, 2020[9]).
All older adults should undertake regular physical activity. Older adults should do at least 150– 300 minutes of moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity during the week, for major health benefits. For additional health benefits older adults should do muscle strengthening activities at moderate or greater intensity that involve all major muscle groups on two or more days a week. They may also increase moderate intensity aerobic physical activity to more than 300 minutes; or do more than 150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous intensity activity, during the week. As part of their weekly physical activity, to enhance functional capacity and to prevent falls, older adults should do varied multicomponent physical activity that emphasises functional balance and strength training at moderate or greater intensity, on 3 or more days a week. Older adults should also limit the amount of time spent being sedentary (WHO, 2020[9]).
It is recommended that all pregnant and postpartum women without contraindication should engage in regular physical activity throughout pregnancy and postpartum. Women should do at least 150 minutes of moderate intensity aerobic physical activity during the week for major health benefits. For additional health benefits include a variety of aerobic and muscle strengthening activities and gentle stretching. In addition, women who before pregnancy engaged regularly in vigorous intensity aerobic activity, or who were physically active, can continue these activities during pregnancy and the postpartum period. Pregnant and postpartum women should limit the amount of time spent being sedentary (WHO, 2020[9]).
Adults and older adults with chronic conditions (cancer, hypertension, type 2 diabetes and HIV) should do at least 150-300 minutes of moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous intensity activity throughout the week, for substantial health benefits. For additional health benefits, they should also do muscle-strengthening activities at moderate or greater intensity that involve all major muscle groups on 2 or more days a week. To enhance functional capacity and to prevent falls, they should do varied multicomponent physical activity that emphasises functional balance and strength training at moderate or greater intensity, on 3 or more days a week.
When not contraindicated, adults and older adults with these chronic conditions may increase moderate intensity aerobic physical activity to more than 300 minutes; or do more than 150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous intensity activity throughout the week for additional health benefits (WHO, 2020[9]).
This age group living with disability should do at least an average of 60 minutes per day of moderate- to vigorous intensity, mostly aerobic, physical activity, during the week, including at least 3 sessions per week of vigorous-intensity aerobic activities, as well as those that strengthen muscle and bone (WHO, 2020[9]).
Adults living with disability should do at least 150-300 minutes of moderate-intensity aerobic physical activity; or at least 75-150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity, during the week, for major health benefits. For additional health benefits, adults living with disability should also do muscle-strengthening activities at moderate or greater intensity that involve all major muscle groups, on 2 or more days a week. They may increase moderate-intensity aerobic physical activity to more than 300 minutes; or do more than 150 minutes of vigorous-intensity aerobic physical activity; or an equivalent combination of moderate- and vigorous-intensity activity throughout the week. To enhance functional capacity and to prevent falls, older adults should do varied multicomponent physical activity that emphasises functional balance and strength training at moderate or greater intensity, on 3 or more days a week (WHO, 2020[9]).