
Pregnancy and birth
Antenatal care, delivery attended by skilled health professionals and access to health facilities for delivery are important for the health of both mothers and their babies as they reduce the risk of birth complications and infections (see indicators “Preterm births and low birthweight” and “Infant feeding” in Chapter 4). WHO currently recommends a minimum of eight antenatal visits (WHO, 2016[13]), and antenatal care coverage has been monitored to ensure universal access to sexual and reproductive health care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programmes by 2030 (Sustainable Development Goal 3.7).
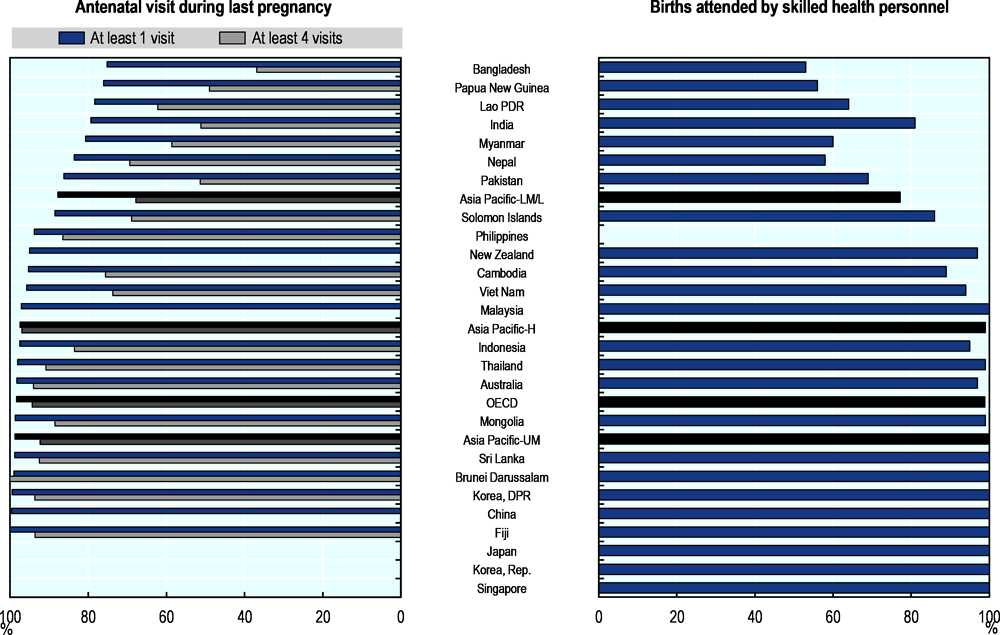
In Asia-Pacific, only two in three pregnant women – on average – received the recommended four visits in lower-middle and low income countries, but access to antenatal care varies across countries (Figure 5.15, left panel). DPR Korea, Sri Lanka, Brunei Darussalam, Fiji, Thailand, and Australia have nearly complete coverage of four antenatal visits. At the other end, in Bangladesh and Papua New Guinea the coverage of four antenatal care visits is less than 50%.
Only three women in four had births attended by a skilled health professional – a doctor, nurse or midwife – in lower-middle and low income Asia-Pacific countries, whereas almost all births were attended by a skilled health professional in high and upper-middle income countries and territories (Figure 5.15, right panel). Less than two births in three in Bangladesh, Lao PDR and Papua New Guinea were attended by a skilled health professional, with most deliveries assisted by dais or untrained birth attendants. Traditional birth attendants are important in several other countries including Cambodia, India, Indonesia, Myanmar, Pakistan and the Philippines, especially in rural settings.
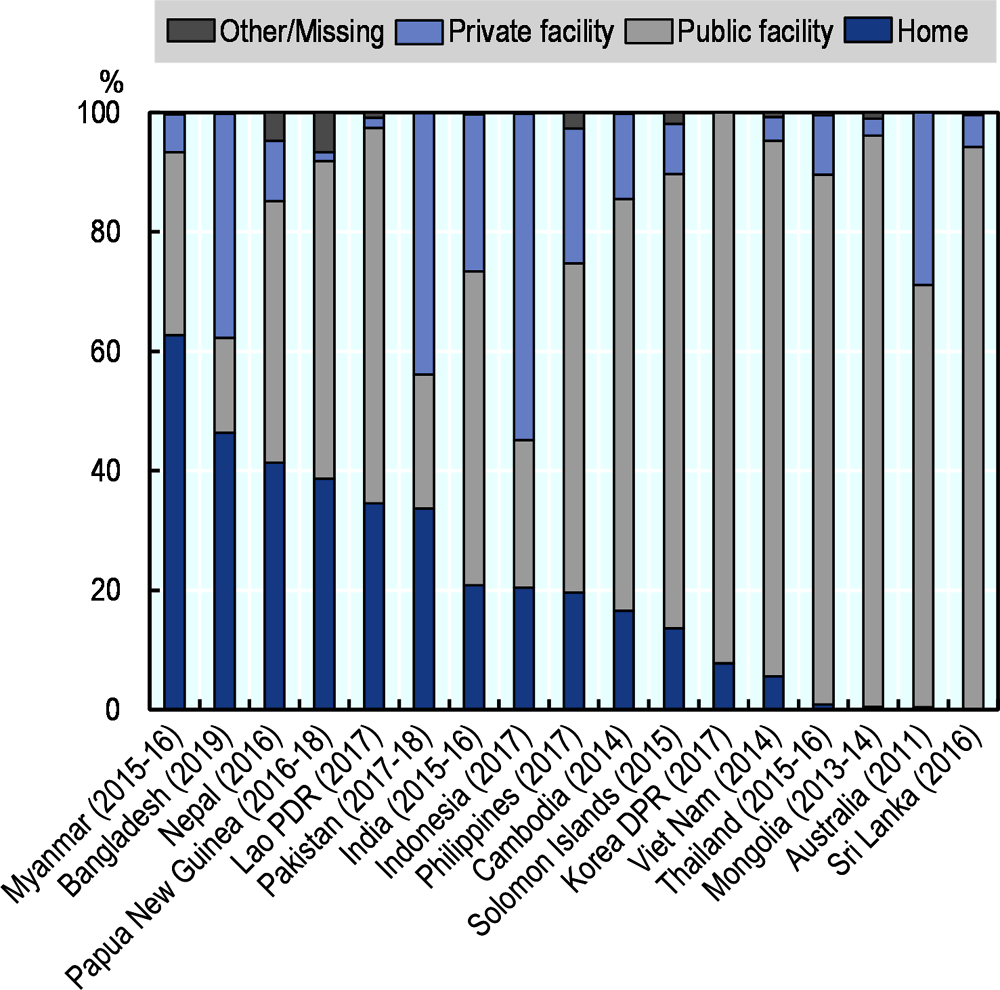
Delivery in health facilities varies across countries (Figure 5.16). In Australia, Thailand, Mongolia, Sri Lanka, DPR Korea and Viet Nam, almost all deliveries take place at a health facility. On the other hand, in Myanmar, most deliveries occur at home and only less than 40% of births takes place in a health facility. Across countries, deliveries in health facilities are more common among mothers giving birth for the first time, or those who have had at least four antenatal visits, as well as among mothers living in urban regions and those with higher education and wealth.
Access to skilled birth attendants varies by socio-economic factors (Figure 5.17). Mongolia, Thailand and Sri Lanka have a high coverage of births attended by skilled health professionals among mothers with different education and income levels, and living in different geographical locations. However, in other countries, the coverage of births attended by skilled health professionals is highly unequal among women of different income and education levels. For example, in Myanmar and Lao PDR, access differs more than three-fold between mothers of the lowest education level and mothers of the highest education levels. Disparity by household income is largest in Myanmar, almost 4-fold difference between mothers living in household at the highest and at the lowest income quintiles, and in the Philippines and Lao PDR, a 3-fold difference. In contrast, differences in access to skilled care at birth remain relatively small between urban and rural areas across countries (except in Myanmar and Lao PDR).
The major source of information on care during pregnancy and birth are health interview surveys. Demographic and Health Surveys (DHS), for example, are nationally representative household surveys that provide data for a wide range of indicators in the areas of population, health, and nutrition. Standard DHS Surveys have large sample sizes (usually between 5 000 and 30 000 households) and typically are conducted every five years, to allow comparisons over time. Women who had a live birth in the five years preceding the survey are asked questions about the birth, including how many antenatal care visits they had, who provided assistance during delivery, and where the delivery took place.
Source: WHO GHO 2020; UNICEF 2020.
Source: DHS and MICS surveys, various years.
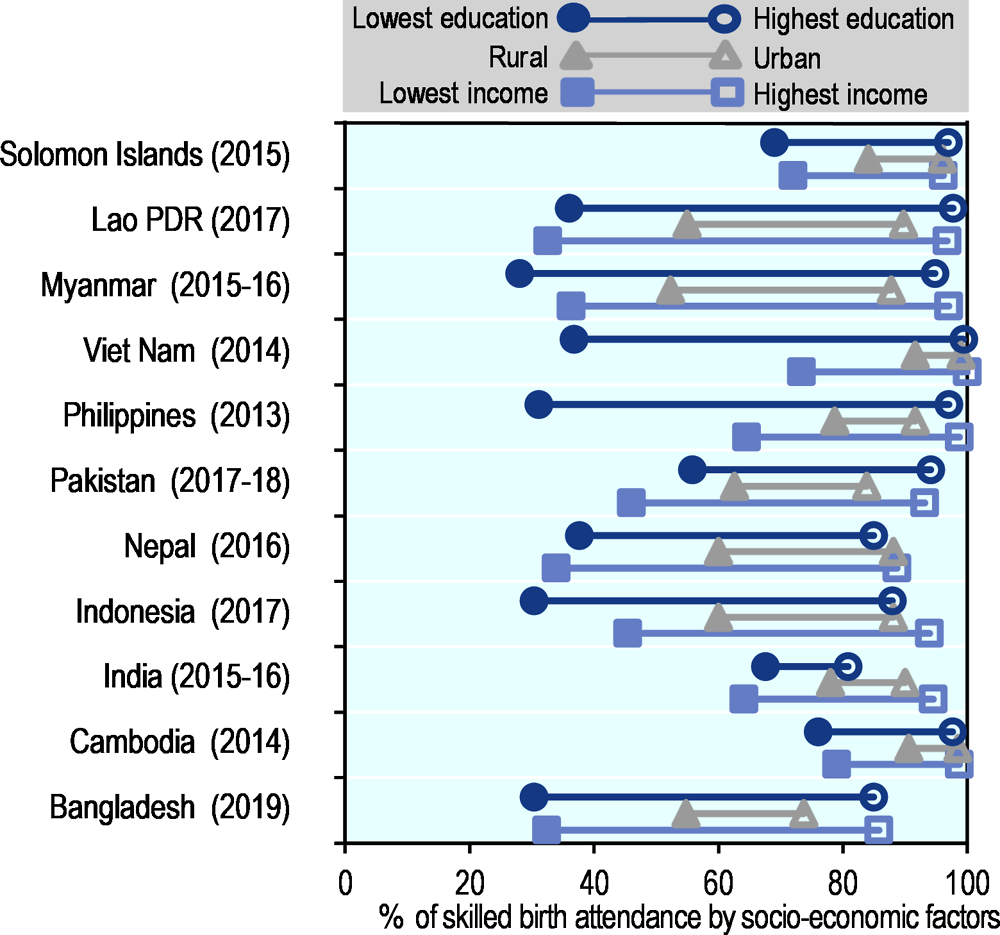
Note: Mongolia, Singapore, and Thailand are not shown as they have > 95% of births attended by skilled health professionals across all socio-economic and geographical groups.
Source: DHS and MICS surveys, various years.