
copy the linklink copied!Chapter 3. Trends in children’s emotional well-being
Emotional well-being is vital for our health and everyday life. A large body of research documents the long-term benefits of developing social and emotional skills and a positive mental health state during childhood and adolescence. These are crucial developmental periods and research demonstrates that they can be important predictors of emotional well-being later in life since many adult mental health disorders originate during this period. This chapter will provide an overview of some of the long-term trends and challenges in children's emotional well-being, including internalising (e.g. anxiety and depression) and externalising behaviours (e.g. bullying and cyberbullying). It will also look specifically at policy priorities and challenges faced by OECD countries and systems.
copy the linklink copied!Why is emotional well-being so important?
Emotional well-being is vital for our health and everyday life. It is an important element of our overall well-being (Pollard and Lee, 2003[1]), happiness and confidence, and is essential for a "good quality of life" (Morgan et al., 2007[2]). A large body of research documents the benefits of developing social and emotional skills and positive mental health during the early years and demonstrates how these can be important predictors of emotional well-being later in life. For example, longitudinal data analysis shows that 14-year-olds in Korea who have a high sense of responsibility are less likely to suffer from depression at age 19; kindergarten students in the United States in the top decile of the social and emotional skills distribution are less likely to report that they are depressed in grade 8; and 15- to 19-year-olds in Norway with high levels of self-confidence are less likely to report depression between ages 26 to 31 (OECD, 2015[3]).
Childhood and adolescence are crucial developmental periods. In terms of brain development, these stages of life are when many brain structures and neurosystems are rapidly maturing. This has implications for cognitive functioning, emotion regulation, motivation and social interactions (Paus, Keshavan and Giedd, 2008[4]). In fact, adolescence is increasingly understood to be a sensitive period of development, with both increased developmental opportunities as well as risks, particularly for mental illness (Fuhrmann, Knoll and Blakemore, 2015[5]).
Developmental risks and opportunities in childhood have implications for future well-being outcomes. There is significant evidence that adult mental health disorders can originate during childhood or adolescence (Paus, Keshavan and Giedd, 2008[4]; Kieling et al., 2011[6]; Jones, 2013[7]; WHO, 2017[8]). For example, nearly one in two adult mental health problems begin by age 14 and 75% by the mid-20s (WHO, 2017[8]). However treatment usually does not begin until later due to stigma, lack of awareness and other cultural or social norms (Choi, 2018[9]). It is important to examine the causes and contributing factors and to detect mental health problems earlier – before conditions become chronic and serious (Morgan et al., 2007[2]; OECD, 2015[3]).
Defining emotional well-being and mental health
Well-being has become an increasingly popular area of research (Dodge et al., 2012[10]) and policy (Choi, 2018[9]). However, there is little consensus around how it should be defined, with research often focusing on dimensions of well-being rather than a general definition (Dodge et al., 2012[10]). This chapter focuses on emotional well-being, often referred to as "hedonic well-being", which signifies the quality of an individual's emotions and experiences (i.e. sadness, anxiety, worry, happiness, stress depression, anger, joy and affection) that leads to unpleasant or pleasant feelings (Choi, 2018[9]).
Emotional well-being is generally seen as a core component of positive mental health (Westerhof and Keyes, 2010[11]). The World Health Organisation (WHO) defines mental health as "A state of well-being in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community," (2018[12]). Another review outlines two dimensions of mental health: the positive (well-being and coping with difficulties) and the negative (symptoms and disorders). Positive mental health does not solely mean the absence of symptoms like anxiety or depression, but also includes other factors like happiness, self-esteem and balanced emotions (Korkeila et al., 2003[13]).
Despite the importance of emotional well-being, its indicators are not always explicitly included in frameworks for child well-being. This may be due to the challenging nature of defining its scope and measuring its components (Choi, 2018[9]). Part of the reason for this could also be due to the interdependent nature of the different dimensions of overall well-being, since dimensions can affect and be affected by one another (Choi, 2018[9]).
This chapter will provide an overview of recent trends in children's emotional well-being. It will also look specifically at policy priorities and challenges faced by OECD countries and systems.
copy the linklink copied!Mental health and emotional well-being trends among youth
While there has been a significant increase in the number of children and adolescents reporting symptoms of mental health problems and psychiatric disorders over the past few decades (Costello, Copeland and Angold, 2011[15]; Olfson et al., 2014[16]), Table 3.1 shows that other issues are becoming less prevalent. This section will provide an overview of emotional well-being trends in youth.
Mental health issues
Overall, about 10% to 20% of children and adolescents in the world suffer from mental health problems and ill-being (Kieling et al., 2011[6]; Henderson et al., 2017[17]), and evidence suggests that some problems are becoming more prevalent among youth (Choi, 2018[9]). Mental illness has become a worry for adolescent girls in particular, for whom many studies report a concerning increase in mental problems (Bor et al., 2014[18]; Blomqvist et al., 2019[19]).
The increase in prevalence might be due to growing awareness and help-seeking behaviours among youth and their parents, which are related to enhanced screening and diagnosis as well as a broader classification of disorders (Collishaw, 2015[20]). However, the rise in mental health problems among youth may have also captured a true increase in prevalence, particularly as some conditions are difficult to detect and diagnose at earlier ages, meaning that they have been more susceptible to under-reporting (Choi, 2018[9]).
Psychiatric disorders during childhood and adolescence are negatively related to emotional well-being, health and education both in the short and long run (Collishaw, 2015[20]). The recurrence of chronic conditions can also lead to further issues. For example, depression during adolescence is associated with negative physical and mental health outcomes such as suicidal thinking and attempts as well as problems with social functioning (Maughan, Collishaw and Stringaris, 2013[21]).
Stigma, lack of awareness and other social and cultural norms around mental illness during childhood and adolescence can lead to treatment not beginning until later in life. In fact, “stigma and discrimination in relation to mental illnesses have been described as having worse consequences than the conditions themselves” (Thornicroft et al., 2016[22]). This is concerning given that studies suggest that adult mental health disorders mostly originate during childhood or adolescence (Choi, 2018[9]).
Developing awareness around the issue is crucial. One example comes from the Flemish Community of Belgium, which developed national awareness campaigns called Rode Neuzen Dag and Te Gek!? (“it’s ok that you fall occasionally…”) to discuss mental health issues and challenge the stigma. Some education ministries have also integrated discussions around mental health in the curriculum to increase awareness, as in Scotland’s (United Kingdom) Curriculum for Excellence.
It is important to note that as awareness of mental health issues grows there tends to be a corresponding increased demand for treatment. Waitlists for child and adolescent mental health services have significantly grown over the past few years in many jurisdictions, including Scotland (Murphy, 2016[23]) and Ontario (Canada) (Gandhi et al., 2016[24]). For education, this has implications in how and when students with mental health challenges are identified, and how they are supported both in and out of the classroom. This requires involving health care authorities in the planning and implementation processes of intervention policies in order to ensure a comprehensive and coherent response.
Anxiety and depression
There is evidence that the prevalence of anxiety and depression has been increasing since the 1980s in many countries, with more adolescents reporting symptoms in Germany, Greece, Iceland, New Zealand, Norway, People’s Republic of China and Sweden (Choi, 2018[9]). Rates of depression among American adolescents increased from almost 9% to just over 11% between 2005 and 2014 (Mojtabai, Olfson and Han, 2016[25]).
Numerous factors have been associated with depression including “chronic stress related to the pressure to succeed in school, family instability, poverty, sleep deprivation, low self-esteem or self-confidence, and poor social relations with peers, parents and teachers,” as well as bullying (OECD, 2018[26]). Adolescents’ mental health is also an important predictor of educational achievement and mediates the association between poverty and educational achievement (Sznitman, Reisel and Romer, 2011[27]).
Eating disorders and appearance-related social pressure
While research confirms that eating disorders are much less common relative to other mental health problems, they risk becoming serious conditions for affected youth, with girls much more likely than boys to show symptoms (Costello, Copeland and Angold, 2011[15]). Various research studies from different countries ranging from between 1999 and 2013 have found either no change or decreasing prevalence rates of anorexia and bulimia nervosa (Litmanen et al., 2017[28]; Loth et al., 2015[29]; Keski-Rahkonen and Mustelin, 2016[30]), while the proportion of students responding to Health Behaviour in School-Aged Children (HBSC) perceiving their bodies to be too fat has remained stable at 29% between 2001 and 2014 (HBSC Data Management Centre, 2016[14]).
School-related anxiety and stress
A high proportion of 11-, 13- and 15-year-old of students (35%) report feeling some or a lot of pressure from schoolwork, though this proportion has remained stable on average between 2001 and 2014 (WHO, 2016[31]; HBSC Data Management Centre, 2016[14]). This pressure on children comes from peers, parents and teachers, as well as from their personal motivation to excel in their academic achievement. This can manifest itself in worry and anxiety about doing well on exams, getting good grades, and being admitted to post-secondary education programmes, especially in competitive schools (OECD, 2017[32]). This anxiety manifests as a result of their reaction to and interpretation of mistakes made or that they are afraid to make and could be reinforced by factors like a competitive school climate and long study hours. Girls generally report higher school-related anxiety and pressure than boys (OECD, 2017[32]; WHO, 2016[31]). Stressors around academic work and the perception of schoolwork as demanding have also been associated with depressive symptoms (Moksnes et al., 2016[33]), more frequent subjective health complaints and lower levels of life satisfaction (WHO, 2016[31]).
Life satisfaction
Students who reported the highest levels of school-related anxiety also reported lower life satisfaction levels on average across OECD countries in the 2015 Programme for International Student Assessment (PISA) survey (OECD, 2017[32]). Generally, life satisfaction decreases with age, though the decrease between ages 11 and 15 is larger among girls than it is for boys. Overall, life satisfaction is also lower among girls than boys (WHO, 2016[31]; Goldbeck et al., 2007[34]). PISA 2015 confirms this pattern by gender, as girls reported lower average life satisfaction than boys in all countries with available data (OECD, 2017[32]).
Trends over time in reported life satisfaction paint an inconsistent picture, with variations between countries. Using HBSC data from 2002 to 2010, Cavallo and colleagues (2015[35]) identified 12 European and North American countries showing an increase in rates of life satisfaction, 12 with stable rates and 7 with decreasing rates. Overall rates between 2006 and 2014 remained stable (HBSC Data Management Centre, 2016[14]).
Subjective health complaints (e.g. feeling low)
While it is normal for children and adolescents to have subjective health complaints (e.g. headaches, stomach-aches, feeling low, irritability or bad temper) from time to time, these can have a significant negative impact on emotional well-being when experienced regularly and over prolonged periods. Generally, as children grow older, an increasing proportion of them report multiple subjective health complaints at least once per week, with an increase from 13% at age 11 to 21% at age 15 reporting feeling low, for example (WHO, 2016[31]). A meta-analysis of national and international studies from 1982-2013 across 36 countries found that subjective health complaints have remained stable in the 21st century (Potrebny, Wiium and Lundegård, 2017[36]), though many countries have seen an increasing trend in reports of feeling low (Choi, 2018[9]).
In addition to age, socio-economic status and gender are differentially associated with feeling low. Disadvantaged students are more likely to report feeling low than their more affluent peers. Girls are also more likely than boys to report feeling low, and there is a steeper increase with self-reported feeling low associated with age. As of 2014, 29% of girls at age 15 reported feeling low at least once per week versus only 13% of boys (WHO, 2016[31]). Figure 3.1 shows that while the proportion of male adolescents reporting feeling low has remained stable on average between 2006 and 2014, the proportion of 13- and 15-year-old girls has increased.
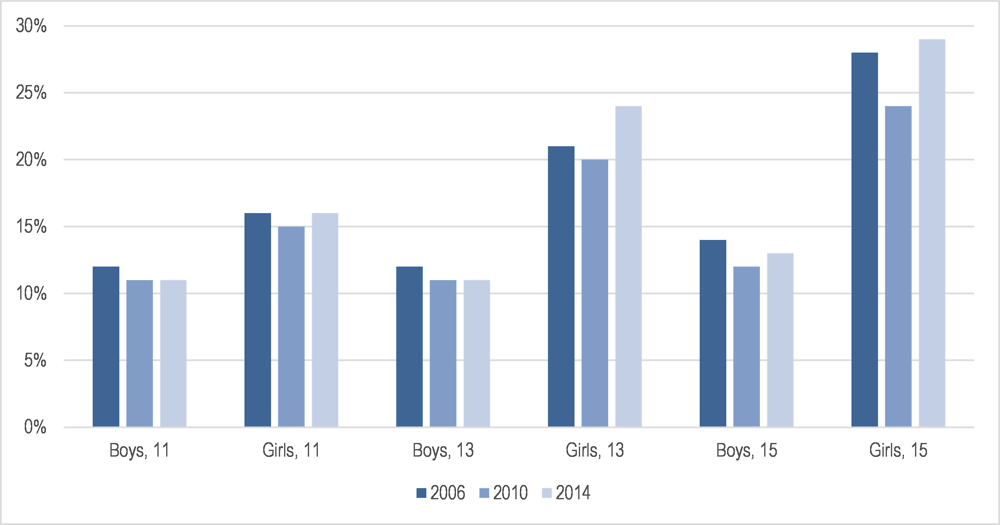
Source: Adapted from HBSC Data Management Centre (2016[14]) and WHO (2016[31])
Note: Prevalence based on unweighted averages for 34 countries that provided data over all three cycles.
Bullying
Rates of bullying and victimisation (both occasional and chronic) have been decreasing in most of the countries with available data between 1994 and 2014, although cross-country variation exists (UNESCO, 2019[37]; HBSC Data Management Centre, 2016[14]). Nonetheless, it remains an important issue: according to PISA 2015 data, 19% of students reported being bullied (all types: relational (i.e. social exclusion), physical (i.e. hitting, punching or kicking), verbal (name-calling or mocking)) at least a few times a month on average across OECD countries. Verbal bullying and relational bullying were the most common forms reported, though there were differences between boys and girls, with boys more likely to report being victims of physical bullying and girls more likely to report being victims of nasty rumours (OECD, 2017[32]). In terms of being the bully, boys significantly more often reported bullying others than girls, according to HBSC data. In addition, on average as age increases being bullied decreases, whereas the opposite is true for being the bully which is more common at age 15 than age 11 (WHO, 2016[31]).
While bullying has been decreasing on average in many OECD countries, it still affects many children in the world and has lasting adverse consequences. Adolescents who are victims or bullies are more likely to have depressive and anxiety symptoms, low self-esteem, feel lonely and lose interest in activities (Kochel, Ladd and Rudolph, 2012[38]; Swearer and Hymel, 2015[39]). Bullying also has negative influences on bystanders who report feelings of guilt or helplessness (Huitsing and Veenstra, 2012[40]; Molcho et al., 2009[41]). These adverse effects can persist into adulthood with consequences such as lower participation in the labour force (Drydakis, 2014[42]).
Certain groups of students are more likely to face challenges for emotional well-being. For example, students identifying as homosexual were three times more likely to be bullied than their heterosexual peers, while students identifying as transgender were five times more likely to experience bullying than their peers in one New Zealand study (Lucassen et al., 2014[43]). A UNESCO review confirms this pattern globally, with proportions as high as 85% of LGBTQ+ (lesbian, gay, bisexual, transgender and queer+) students reporting being bullied in the case of the United States (UNESCO, 2016[44]). Students with disabilities and ethnic minority groups, including Maori and Pacific peoples in New Zealand and indigenous peoples in Australia and Canada, are also more vulnerable to bullying. These students are more prone to other emotional well-being challenges as well, such as mental health issues and are more likely to commit suicide.
These are intersecting issues, and mental health conditions and bullying are contributing factors to higher risks of youth suicide and suicidal thinking among vulnerable youth (McLoughlin, Gould and Malone, 2015[45]; Mueller et al., 2015[46]). This complexity makes finding effective interventions and policy solutions particularly challenging.
Cyberbullying
Bullying has evolved over time, as it takes on new forms and shifts to online spaces in the form of cyberbullying, accompanying the rise in smartphones, social media and other communicative technologies (Choi, 2018[9]). Cyberbullying remains less prevalent than traditional forms of bullying, although is highly correlated with traditional bullying (Modecki et al., 2014[47]). In 2013, between 0% and 12% of youth reported experiencing cyberbullying victimisation (e.g. “mean instant messages, wall-posts, emails and text messages, or creating a web page that made fun of them,” (Choi, 2018[9]; WHO, 2016[31]).
Like traditional bullying, cyberbullying can have serious adverse effects on children’s well-being. Research has highlighted significant relationships between cyberbullying and mental health issues such as anxiety and depression. Cyberbullying has also been related to behavioural challenges such as lack of focus (particularly in school), anger and hostile behaviour, and truancy, which can adversely affect students’ achievement and emotional well-being (Choi, 2018[9]; Tokunaga, 2010[48]). Cyberbullying can also be associated with suicidal thoughts or behaviour (Brailovskaia, Teismann and Margraf, 2018[49]).
Suicide
Adolescent suicide rates have decreased on average since 1990 from 8.5 suicides per 100 000 teenagers (15- to 19-year-olds) to 7.4 in 2015. Much of this decrease occurred in the 2000s. However, some countries have seen worrying increases in teen suicide over this time period such as Japan, Korea, Latvia, Mexico and New Zealand (OECD, 2017[50]).
Tendencies differ among boys and girls, with higher rates of suicide for boys while girls have higher rates of suicidality (i.e. suicidal thoughts, self-harm, suicide attempts and suicide) (McLoughlin, Gould and Malone, 2015[45]). More recently, some countries, such as the United States, have seen an increase in suicides among girls relative to boys, and a greater increase among 10- to 14-year-olds than for 15- to 19-year-olds (Ruch et al., 2019[51]). Ruch and colleagues (2019[51]) argue that this narrowing of the gap could be due to girls using more violent and lethal methods. Research has confirmed a strong link between youth suicide and depression and other mental health problems (Collishaw, 2015[20]; Mojtabai, Olfson and Han, 2016[25]).
copy the linklink copied!Evolving factors influencing emotional well-being outcomes
Changing social and economic conditions
The causal relationship between family poverty and child emotional well-being has been well established (Yoshikawa, Aber and Beardslee, 2012[52]). More broadly, social and economic conditions of a country can also play a role in children's emotional well-being by affecting individual families and their overall financial resources as well as external and internal pressure and concerns about the future (Ottova-Jordan et al., 2015[53]).
Many OECD countries experienced economic growth and prosperity over the past decades. However, income inequality has also increased between and within countries (OECD, 2019[54]). While higher family incomes are generally associated with higher life satisfaction and lower levels of negative emotional experiences (Kahneman and Deaton, 2010[55]), this association is weaker in countries with higher income inequality (Ng and Diener, 2019[56]). This pattern holds true for 15-year-olds across OECD countries, with those whose relative family wealth was lower than that of their peers at school reporting significantly lower life satisfaction levels even after accounting for socio-economic status (OECD, 2017[32]). Analysis using HBSC data also shows that exposure to income inequality during early childhood (0-4 years) predicted lower life satisfaction and psychosomatic symptoms for female adolescents (Elgar et al., 2017[57]).
Increasing migration
As OECD countries experience an increasing flow of migration, children in these countries are more likely to meet and interact with peers and teachers from different cultural backgrounds. This may pose new challenges around migrant students’ integration into different school communities (OECD, 2017[32]). For example, due to differences in culture, language, race and ethnicity, first generation immigrant children face higher rates of bullying victimisation than third generation and native born children (Pottie et al., 2015[58]). Children who arrived as migrants between 13 and 16 years of age are also more likely to report higher levels of bullying victimisation at school than students who arrived earlier (OECD, 2017[32]). Furthermore, children who are forcibly displaced face a number of risk factors for their emotional well-being. Mental health challenges in this population may be compounded by trauma from experiences in their home country, in the displacement itself and in the readjustment to the new context (see Chapter 7).
Changing family structures
Over the last two decades, families have changed on a number of fronts: increasing rates of divorce, older parents, children born outside of marriage and single parent households. The share of divorced or separated parents has increased across many OECD countries and 17% of children lived with a single parent in 2017 (OECD, 2018[59]). Changing families can have implications for children's mental health, emotional well-being and educational achievement. For children with divorced parents, adjustments to changes in financial resources, in parental relationships and involvement, and in levels of family stress and conflict are all negatively associated with emotional well-being and academic achievement (see Box 3.3 for an example of the interactions between a natural disaster, changing families and emotional well-being outcomes). While it would be expected that these associations may be weakened as non-traditional family structures become more common and social stigma decreases, research shows that they have instead remained stable over time (Härkönen, Bernardi and Boertien, 2017[60]).
Severe weather events and natural disasters can significantly increase levels of distress, which strain social relationships, adversely affect mental health and even lead to increased levels of violence.
To deal with the significant mental health issues in the communities affected by the 2010 Canterbury Earthquake and the 2011 aftershock, New Zealand adopted Mana Ake, a programme for children ages 5-12 years old in earthquake-affected communities. It consists of Kaimahi teams, "which have a diverse range of skills and include psychologists, social workers, counsellors, teachers and youth workers." The approach aims for collaboration between support services and clusters of schools and education personnel (including early childhood educators) to target resources most effectively.
The Kaimahi specialists work with teachers and families when children are dealing with ongoing issues that affect their well-being (anxiety, social isolation, parental separation, grief and loss and managing emotions). The specialists are employed by 13 different NGOs. The teams can work with individual students at school, in the community or at home, and with groups of students at school.
In 2018, New Zealand announced its intention to broaden the programme to make Mana Ake available for all primary to lower secondary schoolchildren across Greater Christchurch, the Hurunui and Kaikōura (New Zealand Ministry of Health – Manatū Hauora, 2018[61]), as part of the lead-up to its first Wellbeing budget in 2019 (Government of New Zealand, 2019[62]). Evaluations of the initial waves of Mana Ake suggest the programmes can have significant social outcomes and value for money, as well as a sustainable, intangible and collective impact (Savage et al., 2018[63]).
Changing sleep patterns
Some lifestyle factors of modern childhood, including stress, less time to play and more hours to do school work, mean that children today across OECD countries face higher odds of sleep deprivation (Choi, 2018[9]). Most studies cite evidence of a long-term decline in sleep duration among children and adolescents, although it is not extreme (Matricciani et al., 2017[64]). Having enough sleep is crucial for children’s physical and emotional well-being. Lack of sleep negatively affects children’s mental health and emotional regulation, and is associated with relationship stress and suicidal thinking (Sarchiapone et al., 2014[65]; Chaput et al., 2016[66]). Adolescents with sleep disorders also tend to have lower average health-related quality of life and more subjective health complaints (Paiva, Gaspar and Matos, 2015[67]).
Increasing urbanisation
Nearly half of the world’s population lives in cities (OECD, 2016[68]). This share of the population has been growing, with rural areas seeing increasing population loss (OECD, 2019[54]). While there are potential benefits of urbanisation, it is correlated with a lower sense of social connection and belonging in local communities and neighbourhoods (OECD, 2016[68]), which can worsen social alienation and exclusion. Urban upbringing is also associated with increased risks of mental health problems, as well as substance use and physical inactivity (Patton et al., 2016[69]). Increasing urbanisation also means that more and more children are growing up in built-up environments with less green space. There is some evidence of a positive association between children and adolescents’ mental well-being and exposure to green spaces, a relationship already well documented for adults, though additional research is necessary (Vanaken and Danckaerts, 2018[70]).
copy the linklink copied!Strengthening protective factors
A number of factors can protect children from negative emotional well-being outcomes, even when faced with adverse circumstances. Incorporation of protective factors into the lives of children is important to build resilience (i.e. “the capacity to successfully develop even when faced by chronic adversity and stress” (Barnes, 2016[71])). Personal protective factors such as social and emotional skills (e.g. motivation, self-regulation, autonomy and cooperativeness, self-efficacy and self-worth) are important in strengthening children’s emotional well-being (OECD, 2015[3]). Social and emotional skills can be fostered by forming close and secure relationships with parents during early childhood (see Chapter 4), and programmes to develop them in school are often incorporated into national curricula. Relationships not only help bolster children’s social and emotional skills; stable emotional support can act as a protective or compensatory factor when dealing with challenges to emotional well-being such as chronic stress, exposure to bullying and depression (OECD, 2015[3]; OECD, 2017[32]; Goldman et al., 2016[72]).
Effective prevention and intervention programmes in schools can help reduce and prevent anxiety and depression as well as increase the awareness of different mental health issues among youth (Choi, 2018[9]). One of the most common components found among prevention programmes for adolescent depression, anxiety and suicide is cognitive-behavioural therapy (CBT). These types of programmes focus on cognitive and behavioural risk factors among children and teach children and adolescents cognitive restructuring skills that help them detect and overcome negative thoughts and emotions as well as improve their problem solving skills (Das et al., 2016[73]; Choi, 2018[9]).
In a recent review of existing studies on prevention programmes for mental health, substance use, violence, sexual health and life skills, problem solving was the most commonly shared practice element (76% of the programmes), followed by communication skills (45%), assertiveness (45%) and insight building (38%). Along with a growing body of evidence, these commonalities among prevention programmes all indicate the importance of social and emotional skills as a powerful tool to counteract and overcome the adverse effects of mental health problems (Choi, 2018[9]).
As mentors, educators and role models, teachers also have an important role in strengthening emotional well-being in students (OECD, 2015[3]). Students who have good relationships with their teachers tend to be happier and those who report high levels of support from their teachers tend to handle stress better at school (Malecki and Demaray, 2006[74]; Goldman et al., 2016[72]). Positive teacher-student relationships are also associated with better emotion regulation and positive peer relationships (Goldman et al., 2016[72]), as well as reduction in behaviours such as suicidal thoughts, substance use and violence (Bergin and Bergin, 2009[75]). Inversely, negative teacher-student relationships can make students more vulnerable to challenges. For example, students’ perceptions of unfair treatment by their teacher and of the school disciplinary climate have been identified as some of the strongest predictors of bullying victimisation (OECD, 2017[32]).
Open communication and exchange of information between parents, teachers and students when implementing intervention programmes is crucial for children who are being bullied at school or experiencing mental health issues. This is especially pertinent as many parents are not aware of the difficulties their children face and cite lack of information on how to be involved in schools or on how their involvement would help their child's development as communication obstacles (Choi, 2018[9]). Raising awareness among youth for mental health issues like depression, anxiety and eating disorders is crucial early on so that they do not become severe and chronic (Gladstone, Beardslee and O’Connor, 2011[76]), especially since a majority of youth with these problems do not get or seek out treatment (Choi, 2018[9]). Youth with the highest need are often those who do not seek support and who have the least access to help or treatment, which compounds the difficulty (McLoughlin, Gould and Malone, 2015[45]).
Many countries have developed strategic policy frameworks that address emotional well-being challenges in holistic well-being frameworks. These tend to address multiple challenges through a comprehensive approach, often focusing on both preventing and limiting the effects of different issues. Research generally confirms that ‘whole-school’, ‘comprehensive’, or ‘school and system-wide interventions’, that look at both prevention and response are effective (Richard, Schneider and Mallet, 2012[77]; UNESCO, 2017[78]).
copy the linklink copied!Considerations for future research
Despite the presence of large-scale international surveys with indicators on emotional well-being, most independent studies and data sets are quite limited because they tend to have small samples, are conducted in developed countries and are mostly cross-sectional in design (Choi, 2018[9]). Future research should focus on strengthening this base. Current gaps and areas in need of further research include:
-
There is a rarity of representative data samples from childhood into adolescence and from adolescence into adulthood necessary for understanding the change and persistence of psychiatric disorders and other emotional well-being factors.
-
There is a need for up-to-date data on cyberbullying and other challenges among younger children to understand the long-term relationships and trends. Most cross-national data are from large-scale assessments that survey adolescents.
-
Different psychiatric disorders and emotional problems tend to have overlapping causes, symptoms and consequences. Thus, future studies should consider examining multiple outcomes and indicators (i.e. examine the combined effects of stress, anxiety and depression and not each independently), to maximise the understanding how to improve awareness and reduce negative consequences.
-
Further research is necessary to investigate how protective factors, particularly the roles of parents and teachers, can be strengthened in the context of larger well-being framework policy approaches increasingly being adopted.
-
Teachers play a vital role in delivering prevention and intervention programmes (Durlak et al., 2011[79]; Neil and Christensen, 2009[80]). Future research should assess the effectiveness of training programmes to help teachers identify early signs and symptoms of mental health and emotional problems (Choi, 2018[9]), and the practicality of implementation (i.e. cost, additional burden on teachers and necessary support needed to carry out training and programmes).
-
Research on how to involve parents in prevention, detection and intervention programmes effectively is required, particularly in cases of high-risk students. Ways to promote communication and collaboration between teachers and parents online and through emerging virtual well-being hubs should also be investigated.
copy the linklink copied!High priority challenges in OECD countries and systems
Policy makers have taken more interest in the well-being of individuals, particularly children and adolescents, over the past few decades (Choi, 2018[9]). In the 21st Century Children Policy Questionnaire, countries identified a range of issues that they face in their national or regional context that adversely affect children’s emotional well-being, as well as the most pressing challenges in terms of policy priorities. These are presented in Table 3.2.
Bullying was the most common policy concern, flagged by 23 of the 24 countries that responded to this part of the Policy Questionnaire. School-related anxiety and stress and mental illness were also widespread challenges. Bullying was perceived as the most intense, seen as both very prevalent and very pressing. Mental illness and school-based anxiety and stress were also perceived as both highly pressing and prevalent.
While countries often cited trends in international survey data when identifying the most pressing challenges, this was not always the case. Indeed, country-specific issues also influenced perceptions of the challenges and of their intensity. Several countries cited highly mediatised cases around certain challenges like cyberbullying, mental health and suicide, in spite of their suicide rates dropping, for example. Others, like Greece, highlighted the influence of macro-level factors such as the repercussions of the 2008 economic crisis (such as parents not having as much time to spend with their children due to having to work several jobs) on life satisfaction.
Further analysis also indicated that countries selected the same issues but for different reasons due to local or context-specific issues. This was the case for fear and anxiety of threats, for example, with the United States attributing the challenge to the prevalence of gun violence, whereas Turkey cited geopolitical tensions. This shows that while international indicators can help identify trends, contextual and qualitative analysis is also crucial to develop a more nuanced understanding of the underlying causes.
The challenges to children and adolescents’ emotional well-being are often not independent. Many countries noted intersections and relationships between the pressing challenges in their responses, which they often selected together. Figure 3.2 provides a visual depiction of the relative importance and linkages indicated between the challenges.
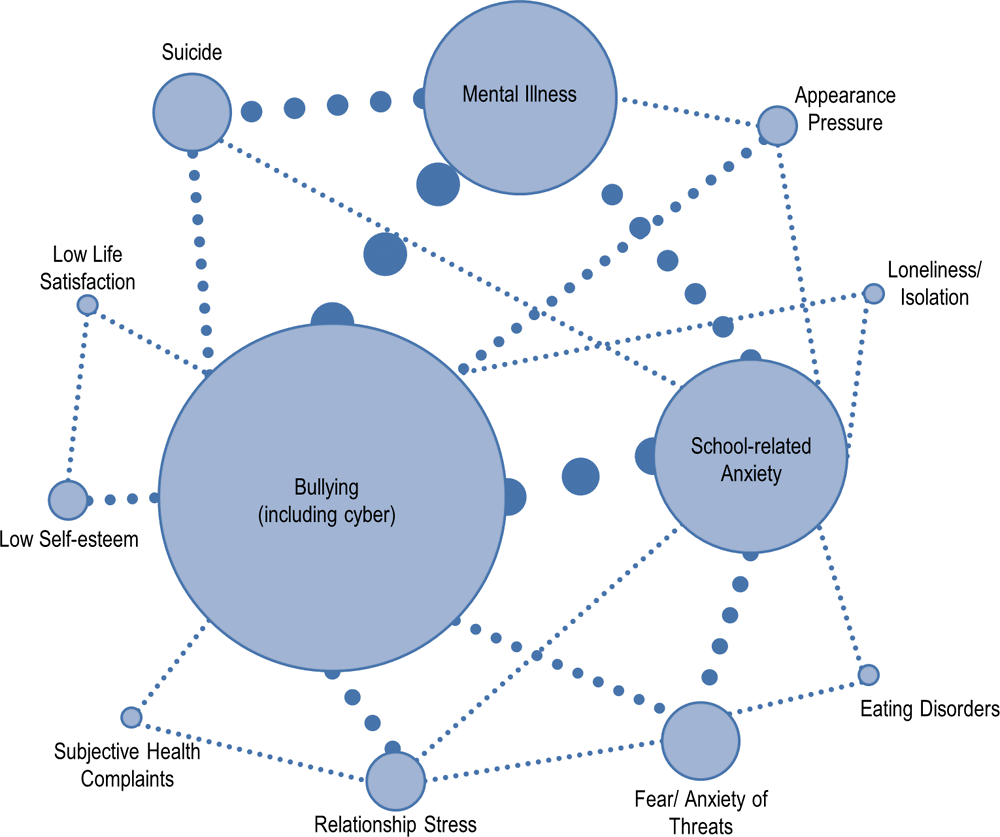
Source: 21st Century Children Policy Questionnaire
Note: Countries and systems were limited to three issues they could flag as “most pressing”. The width of the connectors reflects the number of times the respective challenges were selected together. The size of the circles reflects the number of times each challenge was selected as pressing.
Suicide was often selected with mental health and with bullying, for example. School-based stress was also often selected with mental health, and relationship stress with bullying. Relationships between these challenges on an individual level are confirmed by the literature (Choi, 2018[9]). While countries were asked to select the challenges independently, patterns in the responses suggest the challenges often selected together may also be interrelated on a larger, system-wide scale.
copy the linklink copied!In sum
While there has been a significant increase in children reporting some mental health problems in the 21st century, the prevalence of other emotional well-being challenges has been decreasing. This highlights both the success of some existing efforts to improve children’s emotional well-being as well as some of the challenges that should be prioritised, especially improving the emotional well-being outcomes of girls and children from disadvantaged and migrant backgrounds.
Developing effective policy initiatives is crucial given the interdependent relationship between mental and physical health and overall well-being, as well as because emotional well-being in childhood is also a predictor of emotional well-being later in life. New data, policies and programmes are necessary to more effectively monitor and strengthen children's emotional well-being and protective factors in the short and long run.
copy the linklink copied!Note
The WHO’s Health Behaviour in School-Aged Children (HBSC) study is a collaborative cross-sectional study across 43 countries. HBSC collects data every 4 years among 11, 13, and 15-year-olds through self-reported questionnaires on key health indicators and outcomes, behaviours and background variables. The most recent study from 2013-14 surveyed 220 000 children and adolescents.
References
[71] Barnes, A. (2016), “Childhood stress and resilience”, in Health Promotion for Children and Adolescents, Springer US, Boston, MA, https://doi.org/10.1007/978-1-4899-7711-3_5.
[75] Bergin, C. and D. Bergin (2009), “Attachment in the classroom”, Educational Psychology Review, Vol. 21/2, pp. 141-170, https://doi.org/10.1007/s10648-009-9104-0.
[19] Blomqvist, I. et al. (2019), “Increase of internalized mental health symptoms among adolescents during the last three decades”, European Journal of Public Health, https://doi.org/10.1093/eurpub/ckz028.
[18] Bor, W. et al. (2014), “Are child and adolescent mental health problems increasing in the 21st century? A systematic review”, Australian & New Zealand Journal of Psychiatry, Vol. 48/7, pp. 606-616, https://doi.org/10.1177/0004867414533834.
[49] Brailovskaia, J., T. Teismann and J. Margraf (2018), “Cyberbullying, positive mental health and suicide ideation/behavior”, Psychiatry Research, Vol. 267, pp. 240-242, https://doi.org/10.1016/J.PSYCHRES.2018.05.074.
[35] Cavallo, F. et al. (2015), “Trends in life satisfaction in European and North-American adolescents from 2002 to 2010 in over 30 countries”, The European Journal of Public Health, Vol. 25/suppl 2, pp. 80-82, https://doi.org/10.1093/eurpub/ckv014.
[66] Chaput, J. et al. (2016), “Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth”, Applied Physiology, Nutrition, and Metabolism, Vol. 41/6 (Suppl. 3), pp. S266-S282, https://doi.org/10.1139/apnm-2015-0627.
[9] Choi, A. (2018), “Emotional well-being of children and adolescents: Recent trends and relevant factors”, OECD Education Working Papers, No. 169, OECD Publishing, Paris, https://dx.doi.org/10.1787/41576fb2-en.
[20] Collishaw, S. (2015), “Annual Research Review: Secular trends in child and adolescent mental health”, Journal of Child Psychology and Psychiatry, Vol. 56/3, pp. 370-393, https://doi.org/10.1111/jcpp.12372.
[15] Costello, E., W. Copeland and A. Angold (2011), “Trends in psychopathology across the adolescent years: What changes when children become adolescents, and when adolescents become adults?”, Journal of Child Psychology and Psychiatry, Vol. 52/10, pp. 1015-1025, https://doi.org/10.1111/j.1469-7610.2011.02446.x.
[73] Das, J. et al. (2016), “Interventions for adolescent mental health: An overview of systematic reviews”, Journal of Adolescent Health, Vol. 59/4, pp. S49-S60, https://doi.org/10.1016/J.JADOHEALTH.2016.06.020.
[10] Dodge, R. et al. (2012), “The challenge of defining wellbeing”, International Journal of Wellbeing, Vol. 2/3, http://internationaljournalofwellbeing.org/ijow/index.php/ijow/article/view/89.
[42] Drydakis, N. (2014), “Bullying at school and labour market outcomes”, International Journal of Manpower, Vol. 35/8, pp. 1185-1211, https://doi.org/10.1108/ijm-08-2012-0122.
[79] Durlak, J. et al. (2011), “The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions”, Child Development, Vol. 82/1, pp. 405-432, https://doi.org/10.1111/j.1467-8624.2010.01564.x.
[57] Elgar, F. et al. (2017), “Early-life income inequality and adolescent health and well-being”, Social Science & Medicine, Vol. 174, pp. 197-208, https://doi.org/10.1016/J.SOCSCIMED.2016.10.014.
[5] Fuhrmann, D., L. Knoll and S. Blakemore (2015), “Adolescence as a sensitive period of brain development”, Trends in Cognitive Sciences, Vol. 19/10, pp. 558-566, https://doi.org/10.1016/J.TICS.2015.07.008.
[24] Gandhi, S. et al. (2016), “Mental health service use among children and youth in Ontario: Population-based trends over time”, The Canadian Journal of Psychiatry, Vol. 61/2, pp. 119-124, https://doi.org/10.1177/0706743715621254.
[76] Gladstone, T., W. Beardslee and E. O’Connor (2011), “The prevention of adolescent depression”, Psychiatric Clinics of North America, Vol. 34/1, pp. 35-52, https://doi.org/10.1016/J.PSC.2010.11.015.
[34] Goldbeck, L. et al. (2007), Life Satisfaction Decreases during Adolescence, Springer, https://doi.org/10.2307/27641333.
[72] Goldman, E. et al. (2016), “Child mental health: Recent developments with respect to risk, resilience, and interventions”, in Health Promotion for Children and Adolescents, Springer US, Boston, MA, https://doi.org/10.1007/978-1-4899-7711-3_6.
[62] Government of New Zealand (2019), Budget 2019: Focus on wellbeing, www.budget.govt.nz/budget/2019/wellbeing/mental-health/supporting-young-people.htm.
[60] Härkönen, J., F. Bernardi and D. Boertien (2017), “Family dynamics and child outcomes: An overview of research and open questions”, European Journal of Population, Vol. 33/2, pp. 163-184, https://doi.org/10.1007/s10680-017-9424-6.
[14] HBSC Data Management Centre (2016), Open Access - HBSC Data Portal - 2001/2002 to 2013/2014, University of Bergen, www.uib.no/en/hbscdata/113290/open-access.
[17] Henderson, J. et al. (2017), “Integrated collaborative care teams to enhance service delivery to youth with mental health and substance use challenges: protocol for a pragmatic randomised controlled trial”, BMJ Open, Vol. 7/2, https://doi.org/10.1136/bmjopen-2016-014080.
[40] Huitsing, G. and R. Veenstra (2012), “Bullying in classrooms: Participant roles from a social network perspective”, Aggressive Behavior, Vol. 38/6, pp. 494-509, https://doi.org/10.1002/ab.21438.
[7] Jones, P. (2013), “Adult mental health disorders and their age at onset”, British Journal of Psychiatry, Vol. 202/s54, pp. s5-s10, https://doi.org/10.1192/bjp.bp.112.119164.
[55] Kahneman, D. and A. Deaton (2010), “High income improves evaluation of life but not emotional well-being.”, Proceedings of the National Academy of Sciences of the United States of America, Vol. 107/38, pp. 16489-93, https://doi.org/10.1073/pnas.1011492107.
[30] Keski-Rahkonen, A. and L. Mustelin (2016), “Epidemiology of eating disorders in Europe”, Current Opinion in Psychiatry, Vol. 29/6, pp. 340-345, https://doi.org/10.1097/YCO.0000000000000278.
[6] Kieling, C. et al. (2011), “Child and adolescent mental health worldwide: Evidence for action”, The Lancet, Vol. 378/9801, pp. 1515-1525, https://doi.org/10.1016/s0140-6736(11)60827-1.
[38] Kochel, K., G. Ladd and K. Rudolph (2012), “Longitudinal associations among youth depressive symptoms, peer victimization, and low peer acceptance”, Child Development, Vol. 83/2, pp. 637-650, https://doi.org/10.1111/j.1467-8624.2011.01722.x.
[13] Korkeila, J. et al. (2003), “Review Article: Establishing a set of mental health indicators for Europe”, Scandinavian Journal of Public Health, Vol. 31/6, pp. 451-459, https://doi.org/10.1080/14034940210165208.
[28] Litmanen, J. et al. (2017), “Are eating disorders and their symptoms increasing in prevalence among adolescent population?”, Nordic Journal of Psychiatry, Vol. 71/1, pp. 61-66, https://doi.org/10.1080/08039488.2016.1224272.
[29] Loth, K. et al. (2015), “Disordered eating and psychological well-being in overweight and nonoverweight adolescents: Secular trends from 1999 to 2010”, International Journal of Eating Disorders, Vol. 48/3, pp. 323-327, https://doi.org/10.1002/eat.22382.
[43] Lucassen, M. et al. (2014), Youth’ 12: The Health and Wellbeing of Secondary School Students in New Zealand. Results for Young People Attracted to the Same Sex or Both Sexes, http://oro.open.ac.uk/43995/1/Same%20Sex%20Report_14NM.pdf.
[74] Malecki, C. and M. Demaray (2006), “Social support as a buffer in the relationship between socioeconomic status and academic performance”, School Psychology Quarterly, Vol. 21/4, pp. 375-395, https://doi.org/10.1037/h0084129.
[64] Matricciani, L. et al. (2017), “Past, present, and future: Trends in sleep duration and implications for public health”, Sleep Health, Vol. 3/5, pp. 317-323, https://doi.org/10.1016/J.SLEH.2017.07.006.
[21] Maughan, B., S. Collishaw and A. Stringaris (2013), “Depression in childhood and adolescence”, Journal of the Canadian Academy of Child and Adolescent Psychiatry / Journal de l’Academie canadienne de psychiatrie de l’enfant et de l’adolescent, Vol. 22/1, pp. 35-40, www.ncbi.nlm.nih.gov/pubmed/23390431.
[45] McLoughlin, A., M. Gould and K. Malone (2015), “Global trends in teenage suicide: 2003–2014”, QJM, Vol. 108/10, pp. 765-780, https://doi.org/10.1093/qjmed/hcv026.
[47] Modecki, K. et al. (2014), “Bullying prevalence across contexts: A meta-analysis measuring cyber and traditional bullying”, Journal of Adolescent Health, Vol. 55/5, pp. 602-611, https://doi.org/10.1016/J.JADOHEALTH.2014.06.007.
[25] Mojtabai, R., M. Olfson and B. Han (2016), “National trends in the prevalence and treatment of depression in adolescents and young adults”, Pediatrics, Vol. 138/6, https://doi.org/10.1542/peds.2016-1878.
[33] Moksnes, U. et al. (2016), “The association between school stress, life satisfaction and depressive symptoms in adolescents: Life satisfaction as a potential mediator”, Social Indicators Research, Vol. 125/1, pp. 339-357, https://doi.org/10.1007/s11205-014-0842-0.
[41] Molcho, M. et al. (2009), “Cross-national time trends in bullying behaviour 1994–2006: Findings from Europe and North America”, International Journal of Public Health, Vol. 54/S2, pp. 225-234, https://doi.org/10.1007/s00038-009-5414-8.
[2] Morgan, A. et al. (2007), Mental Well-being in School-aged Children in Europe: Associations with Social Cohesion and Socioeconomic Circumstances, www.euro.who.int/__data/assets/pdf_file/0006/74751/Hbsc_Forum_2007_mental_well-being.pdf.
[46] Mueller, A. et al. (2015), “Suicide ideation and bullying among US adolescents: Examining the intersections of sexual orientation, gender, and race/ethnicity.”, American journal of public health, Vol. 105/5, pp. 980-5, https://doi.org/10.2105/AJPH.2014.302391.
[23] Murphy, R. (2016), Child and Adolescent Mental Health - Trends and Key Issues, SPICe: The Information Centre, www.parliament.scot/ResearchBriefingsAndFactsheets/S5/SB_16-76_Child_and_Adolescent_Mental_Health_Trends_and_Key_Issues.pdf.
[80] Neil, A. and H. Christensen (2009), “Efficacy and effectiveness of school-based prevention and early intervention programs for anxiety”, Clinical Psychology Review, Vol. 29/3, pp. 208-215, https://doi.org/10.1016/j.cpr.2009.01.002.
[61] New Zealand Ministry of Health – Manatū Hauora (2018), Mental health workers begin in Canterbury schools, New Zealand Ministry of Health, www.health.govt.nz/news-media/news-items/mental-health-workers-begin-canterbury-schools.
[56] Ng, W. and E. Diener (2019), “Affluence and subjective well-being: Does income inequality moderate their associations?”, Applied Research in Quality of Life, Vol. 14/1, pp. 155-170, https://doi.org/10.1007/s11482-017-9585-9.
[54] OECD (2019), Trends Shaping Education 2019, OECD Publishing, Paris, https://dx.doi.org/10.1787/trends_edu-2019-en.
[59] OECD (2018), Children in Families, OECD Family Database, www.oecd.org/els/family/database.htm.
[26] OECD (2018), How is Depression Related to Education?, OECD Publishing, Paris, https://dx.doi.org/10.1787/eag-2017-en.
[32] OECD (2017), PISA 2015 Results (Volume III): Students’ Well-Being, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264273856-en.
[50] OECD (2017), Teenage Suicides (15-19 years old), OECD Family Database, www.who.int/classifications/icd/en/.
[68] OECD (2016), Trends Shaping Education 2016, OECD Publishing, Paris, https://dx.doi.org/10.1787/trends_edu-2016-en.
[3] OECD (2015), Skills for Social Progress: The Power of Social and Emotional Skills, OECD Skills Studies, OECD Publishing, Paris, https://dx.doi.org/10.1787/9789264226159-en.
[16] Olfson, M. et al. (2014), “National trends in the mental health care of children, adolescents, and adults by office-based physicians”, JAMA Psychiatry, Vol. 71/1, p. 81, https://doi.org/10.1001/jamapsychiatry.2013.3074.
[53] Ottova-Jordan, V. et al. (2015), “Trends in multiple recurrent health complaints in 15-year-olds in 35 countries in Europe, North America and Israel from 1994 to 2010”, The European Journal of Public Health, Vol. 25/suppl 2, pp. 24-27, https://doi.org/10.1093/eurpub/ckv015.
[67] Paiva, T., T. Gaspar and M. Matos (2015), “Sleep deprivation in adolescents: Correlations with health complaints and health-related quality of life”, Sleep Medicine, Vol. 16/4, pp. 521-527, https://doi.org/10.1016/j.sleep.2014.10.010.
[69] Patton, G. et al. (2016), “Our future: A Lancet commission on adolescent health and wellbeing”, Lancet (London, England), Vol. 387/10036, pp. 2423-78, https://doi.org/10.1016/S0140-6736(16)00579-1.
[4] Paus, T., M. Keshavan and J. Giedd (2008), “Why do many psychiatric disorders emerge during adolescence?”, Nature Reviews Neuroscience, Vol. 9/12, pp. 947-957, https://doi.org/10.1038/nrn2513.
[1] Pollard, E. and P. Lee (2003), “Child well-being: A systematic review of the literature”, Social Indicators Research, Vol. 61/1, pp. 59-78, https://doi.org/10.1023/a:1021284215801.
[36] Potrebny, T., N. Wiium and M. Lundegård (2017), “Temporal trends in adolescents’ self-reported psychosomatic health complaints from 1980-2016: A systematic review and meta-analysis”, PLOS ONE, Vol. 12/11, p. e0188374, https://doi.org/10.1371/journal.pone.0188374.
[58] Pottie, K. et al. (2015), “Do first generation immigrant adolescents face higher rates of bullying, violence and suicidal behaviours than do third generation and native born?”, Journal of Immigrant and Minority Health, Vol. 17/5, pp. 1557-1566, https://doi.org/10.1007/s10903-014-0108-6.
[77] Richard, J., B. Schneider and P. Mallet (2012), “Revisiting the whole-school approach to bullying: Really looking at the whole school”, School Psychology International, Vol. 33/3, pp. 263-284, https://doi.org/10.1177/0143034311415906.
[51] Ruch, D. et al. (2019), “Trends in suicide among youth aged 10 to 19 years in the United States, 1975 to 2016”, JAMA Network Open, Vol. 2/5, p. e193886, https://doi.org/10.1001/jamanetworkopen.2019.3886.
[65] Sarchiapone, M. et al. (2014), “Hours of sleep in adolescents and its association with anxiety, emotional concerns, and suicidal ideation”, Sleep Medicine, Vol. 15/2, pp. 248-254, https://doi.org/10.1016/j.sleep.2013.11.780.
[63] Savage, C. et al. (2018), The Evaluation of Wave 6: Whānau Initiatives for Te Pūtahitanga o Te Waipounamu The Evaluation of Wave Six Whānau Initiatives for Te Pūtahitanga o Te Waipounamu, Ihi Research, https://static1.squarespace.com/static/548669c2e4b0e9c86a08b3ca/t/5b20404f1ae6cf43f6d29056/1528840319694/Wave+6+Evaluation.pdf.
[39] Swearer, S. and S. Hymel (2015), “Understanding the psychology of bullying: Moving toward a social-ecological diathesis–stress model”, American Psychologist, Vol. 70/4, pp. 344-353, https://doi.org/10.1037/a0038929.
[27] Sznitman, S., L. Reisel and D. Romer (2011), “The neglected role of adolescent emotional well-being in national educational achievement: Bridging the gap between education and mental health policies”, Journal of Adolescent Health, Vol. 48/2, pp. 135-142, https://doi.org/10.1016/j.jadohealth.2010.06.013.
[22] Thornicroft, G. et al. (2016), “Evidence for effective interventions to reduce mental-health-related stigma and discrimination”, The Lancet, Vol. 387/10023, pp. 1123-1132, https://doi.org/10.1016/S0140-6736(15)00298-6.
[48] Tokunaga, R. (2010), “Following you home from school: A critical review and synthesis of research on cyberbullying victimization”, Computers in Human Behavior, Vol. 26/3, pp. 277-287, https://doi.org/10.1016/J.CHB.2009.11.014.
[37] UNESCO (2019), Behind the numbers: Ending school violence and bullying, https://unesdoc.unesco.org/ark:/48223/pf0000366483.
[78] UNESCO (2017), School Violence and Bullying: Global Status Report, https://unesdoc.unesco.org/ark:/48223/pf0000246970.
[44] UNESCO (2016), Out in the Open: Education Sector Responses to Violence Based on Sexual Orientation or Gender Identity/Expression: Summary Report, https://unesdoc.unesco.org/ark:/48223/pf0000244652.
[70] Vanaken, G. and M. Danckaerts (2018), “Impact of green space exposure on children’s and adolescents’ mental health: A systematic review”, International Journal of Environmental Research and Public Health, Vol. 15/12, p. 2668, https://doi.org/10.3390/ijerph15122668.
[11] Westerhof, G. and C. Keyes (2010), “Mental illness and mental health: The Two Continua Model across the lifespan”, Journal of Adult Development, Vol. 17/2, pp. 110-119, https://doi.org/10.1007/s10804-009-9082-y.
[12] WHO (2018), Mental Health: Strengthening our Response, www.who.int/en/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
[8] WHO (2017), Child and Adolescent Mental Health, www.who.int/mental_health/maternal-child/child_adolescent/en/.
[31] WHO (2016), Growing up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-being, www.euro.who.int/en/publications/abstracts/growing-up-unequal.-hbsc-2016-study-20132014-survey.
[52] Yoshikawa, H., J. Aber and W. Beardslee (2012), “The effects of poverty on the mental, emotional, and behavioral health of children and youth: Implications for prevention.”, American Psychologist, Vol. 67/4, pp. 272-284, https://doi.org/10.1037/a0028015.
Metadata, Legal and Rights
https://doi.org/10.1787/b7f33425-en
© OECD 2019
The use of this work, whether digital or print, is governed by the Terms and Conditions to be found at http://www.oecd.org/termsandconditions.
