
copy the linklink copied!Avoidable mortality (preventable and treatable)
Indicators of avoidable mortality can provide a general “starting point” to assess the effectiveness of public health and health care systems in reducing premature deaths from various diseases and injuries. However, further analysis is required to assess more precisely different causes of potentially avoidable deaths and interventions to reduce them.
In 2017, almost 3 million premature deaths across OECD countries could have been avoided through better prevention and health care interventions. This amounts to over one quarter of all deaths. Of these deaths, about 1.85 million were considered preventable through effective primary prevention and other public health measures, and over 1 million were considered treatable through more effective and timely health care interventions.
Some cancers that are preventable through public health measures were the main causes of preventable mortality (32% of all preventable deaths), particularly lung cancer (Figure 3.8). Other major causes were external causes of death, such as road accidents and suicide (25%); heart attack, stroke and other circulatory diseases (19%); alcohol and drug-related deaths (9%); and some respiratory diseases such as influenza and chronic obstructive pulmonary disease (8%).
The main treatable cause of mortality is circulatory diseases (mainly heart attack and stroke), which accounted for 36% of premature deaths amenable to treatment. Effective, timely treatment for cancer, such as colorectal and breast cancers, could have averted a further 26% of all deaths from treatable causes. Diabetes and other diseases of the endocrine system (9%) and respiratory diseases such as pneumonia and asthma (9%) are other major causes of premature deaths that are amenable to treatment.
The average aged-standardised mortality rate from preventable causes was 133 deaths per 100 000 people across OECD countries. Premature deaths ranged from under 96 per 100 000 in Israel, Switzerland, Japan, Italy, Spain and Sweden to over 200 in Latvia, Hungary, Lithuania and Mexico (Figure 3.9). Higher rates of premature death in these countries were mainly due to much higher mortality from ischaemic heart disease, accidents and alcohol-related deaths, as well as lung cancer in Hungary.
The mortality rates from treatable causes across OECD countries was much lower, at 75 per 100 000 population. It ranged from less than 50 in Switzerland, Iceland, Norway, Korea, France and Australia, to over 130 deaths per 100 000 people in Latvia, Mexico, Lithuania and Hungary. Ischaemic heart diseases, strokes and some types of treatable cancers (e.g. colorectal and breast cancers) were the main drivers in Latvia, Lithuania and Hungary, countries with some of the highest treatable mortality rates.
Preventable mortality rates were 2.6 times higher among men than among women across OECD countries (197 per 100 000 population for men, compared with 75 for women). Similarly, mortality rates from treatable causes were about 40% higher among men than women, with a rate of 87 per 100 000 population for men compared with 62 for women. These gender gaps are explained by higher mortality rates among men, which are in part linked to different exposure to risk factors such as tobacco smoking (see indicator Main causes of mortality).
Based on the 2019 OECD/Eurostat definitions, preventable mortality is defined as causes of death that can be mainly avoided through effective public health and primary prevention interventions (i.e. before the onset of diseases/injuries, to reduce incidence). Treatable (or amenable) mortality is defined as causes of death that can be mainly avoided through timely and effective health care interventions, including secondary prevention and treatment (i.e. after the onset of diseases, to reduce case-fatality).
The two current lists of preventable and treatable mortality were adopted by the OECD and Eurostat in 2019. The attribution of each cause of death to the preventable or treatable mortality category was based on the criterion of whether it is predominantly prevention or health care interventions that can reduce it. Causes of death that can be both largely prevented and also treated once they have occurred were attributed to the preventable category on the rationale that if these diseases are prevented, there would be no need for treatment. In cases when there was no strong evidence of predominance of preventability or treatability (e.g. ischaemic heart disease, stroke, diabetes), the causes were allocated on a 50%-50% basis to the two categories to avoid double-counting the same cause of death in both lists. The age threshold of premature mortality is set at 74 years for all causes (OECD/Eurostat, 2019[1]).
Data come from the WHO Mortality Database and the mortality rates are age-standardised to the OECD 2010 Standard Population (available at http://oe.cd/mortality).
References
[1] OECD/Eurostat (2019), “Avoidable mortality: OECD/Eurostat lists of preventable and treatable causes of death”, http://www.oecd.org/health/health-systems/Avoidable-mortality-2019-Joint-OECD-Eurostat-List-preventable-treatable-causes-of-death.pdf.
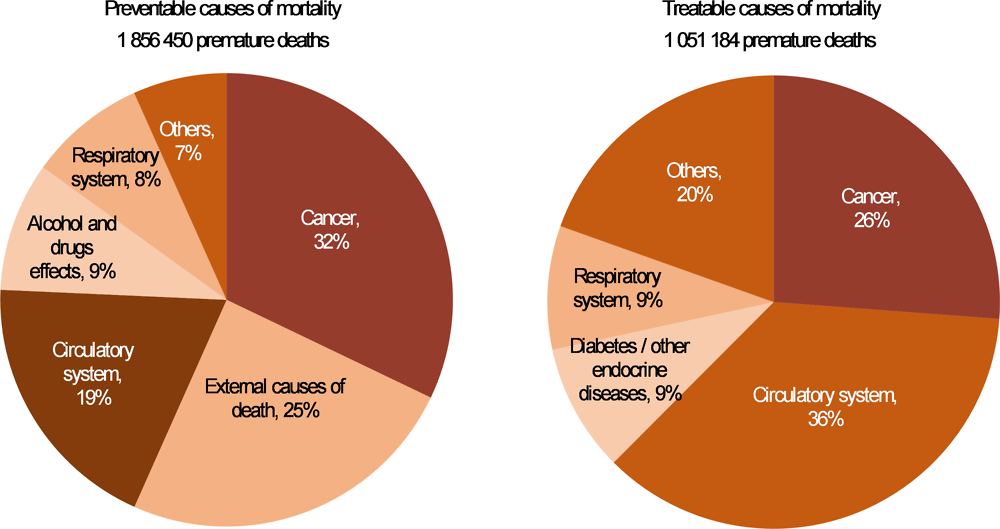
Note: The 2019 OECD/Eurostat list of preventable and treatable causes of death classifies specific diseases and injuries as preventable and/or treatable. For example, lung cancer is classified as preventable; whereas breast and colorectal cancers are classified as treatable.
Source: OECD calculations, based on WHO Mortality Database.
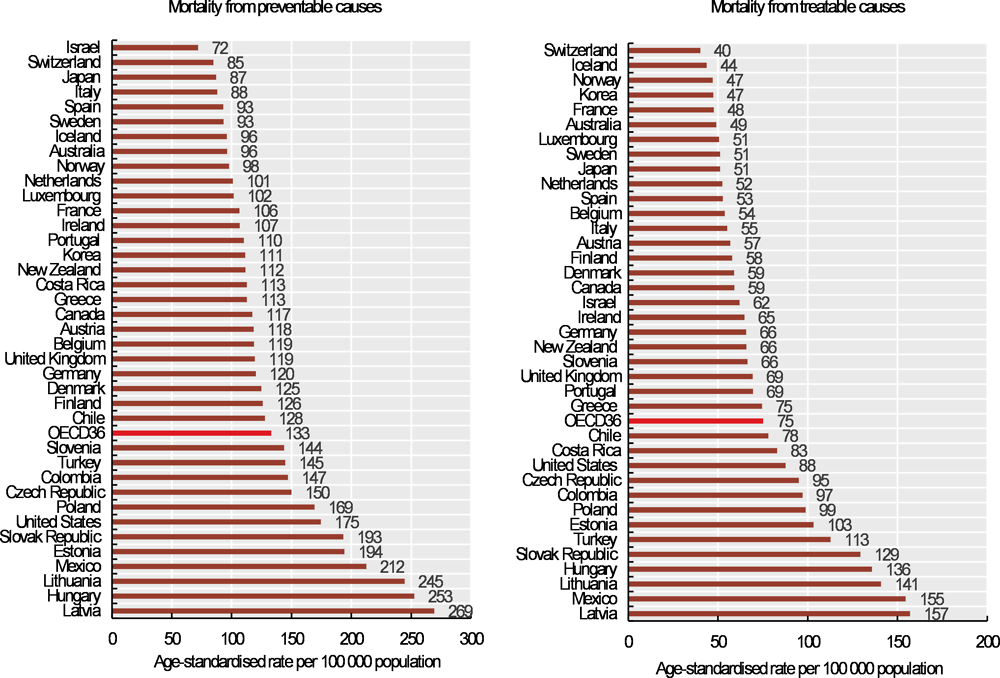
Source: OECD calculations, based on WHO Mortality Database.
Metadata, Legal and Rights
https://doi.org/10.1787/4dd50c09-en
© OECD 2019
The use of this work, whether digital or print, is governed by the Terms and Conditions to be found at http://www.oecd.org/termsandconditions.
